Asuhan Keperawatan trauma dada
51
Asuhan Keperawatan Klien dengan Trauma dada Tuti Herawati, SKp, MN
-
Upload
rini-fauzia-a -
Category
Documents
-
view
705 -
download
11
Transcript of Asuhan Keperawatan trauma dada

Asuhan Keperawatan
Klien dengan Trauma dada
Tuti Herawati, SKp, MN

Introduction
• Struktur Organ: Jantung, pembuluh darah besar, esofagus, trakeobronkial dan paru-paru
• 25% of kematian akibat KLL disebabkan karena trauma dada
• Trauma abdomen umumnya disertai dengan trauma dada
• Penyebab: trauma tumpul dan trauma tajam
• Fokus pencegahan
Sistem yang memperbaiki keselamatan penumpang seperti airbags, safety belt

Anatomi & Fisiologi Thorax
• Tulang dinding thorax– 12 pasang tulang-tulang iga yang berbentuk C
• Ribs 1-7: Join at sternum with cartilage end-points
• Ribs 8-10: Join sternum with combined cartilage at 7th rib
• Ribs 11-12: No anterior attachment
– Sternum• Manubrium
– Joins to clavicle and 1st rib
– Jugular Notch
• Body– Sternal angle (Angle of Louis)
» Junction of the manubrium with the sternal body
» Attachment of 2nd rib
• Xiphoid process– Distal portion of sternum





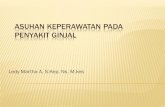
PENYEBAB TRAUMA DADA
• Trauma Tajam
Panah, pisau, handguns,
Shotguns, tergantung jarak
dengan senjata dan kaliber.
Type I: >7 meters: injuri jaringan
lunak
Type II: 3-7 meters : penetrasi
ke fascia dan organ internal
Type III: <3 meters: kerusakan
jaringan yang hebat.
Trauma.org

Penyebab Trauma dada
Trauma Tumpul

Injuri yang menyertai trauma pada
dada• Closed pneumothorax
• Open pneumothorax
(including sucking chest
wound)
• Tension pneumothorax
• Pneumomediastinum
• Hemothorax
• Hemopneumothorax
• Laceration of vascular
structures
• Tracheobronchial tree lacerations
• Esophageal lacerations
• Penetrating cardiac injuries
• Pericardial tamponade
• Spinal cord injuries
• Diaphragm trauma
• Intra-abdominal penetration with associated organ injury


Dinding dada
• Contusion– Umumnya disebabkan trauma tumpul
– Signs & Symptoms• Erythema
• Ecchymosis
• DYSPNEA
• Nyeri saat bernafas
• Suara nafas yang menurun Limited breath sounds
• HYPOVENTILAsi (nyeri saat bernafas)
• Crepitus
• Gerakan dinding dada paradox

Dinding dada
• Fraktur Iga– >50% trauma dada disebabkan oleh trauma tumpul
– Compressional forces flex and fracture ribs at weakest points
– Iga 1-3 diperlukan kekauatan yang besar bila terjadi fraktur, dapat menuebabkan injuri paru
– Iga 4-9 tempat yang paling umum terjadi farktur
– Iga 9-12 jarang terjadi fraktur• Transmisikan energy trauma ke organ internal
• Bila fraktur, curigai adanya injuri hepar dan limpa
– Hypoventilasi umum terjadi karena nyeri


Dinding dada
• Sternal Fracture & Dislocation– Associated with severe blunt anterior trauma
– Typical MOI• Direct Blow (i.e. Steering wheel)
– Incidence: 5-8%
– Mortality: 25-45%• Myocardial contusion
• Pericardial tamponade
• Cardiac rupture
• Pulmonary contusion
– Dislocation uncommon but same MOI as fracture• Tracheal depression if posterior

Dinding dada
• Flail Chest– Segment of the chest that becomes free to move with
the pressure changes of respiration
– Three or more adjacent rib fracture in two or more places
– Serious chest wall injury with underlying pulmonary injury
• Reduces volume of respiration
• Adds to increased mortality
– Paradoxical flail segment movement
– Positive pressure ventilation can restore tidal volume


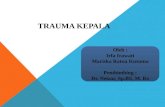
Paradoxical chest wall movement

The point of insertion in the chest most commonly occurs on the
side (lateral thorax), at a line drawn from the armpit (anterior
axillary line) to the side (lateral) of the nipple in males, or to the
side (about 2 in [5 cm]) above the sternoxiphoid junction (lower
junction of the sternum, or chest bone) in females.

Injury Paru-Paru
• Simple Pneumothorax– Closed Pneumothorax
• Progresses into Tension Pneumothorax
– Occurs when lung tissue is disrupted and air leaks into the pleural space
– Progressive Pathology• Air accumulates in pleural space
• Lung collapses
• Alveoli collapse (atelectasis)
• Reduced oxygen and carbon dioxide exchange
• Ventilation/Perfusion Mismatch– Increased ventilation but no alveolar perfusion
– Reduced respiratory efficiency results in HYPOXIA

Injury Paru-Paru
• Open Pneumothorax– Free passage of air between atmosphere and pleural
space
– Air replaces lung tissue
– Mediastinum shifts to uninjured side
– Air will be drawn through wound if wound is 2/3 diameter of the trachea or larger
– Signs & Symptoms• Penetrating chest trauma
• Sucking chest wound
• Frothy blood at wound site
• Severe Dyspnea
• Hypovolemia


Injuri Paru-paru
• Tension Pneumothorax
– Buildup of air under pressure in the thorax.
– Excessive pressure reduces effectiveness of
respiration
– Air is unable to escape from inside the pleural
space
– Progression of Simple or Open Pneumothorax



Pulmonary InjuriesTension Pneumothorax Signs & Symptoms
• Dyspnea
– Tachypnea at first
• Progressive ventilation/perfusion mismatch
– Atelectasis on uninjured side
• Hypoxemia
• Hyperinflation of injured side of chest
• Hyperresonance of injured side of chest
• Diminished then absent breath sounds on injured side
• Cyanosis
• Diaphoresis
• JVD
• Hypotension
• Hypovolemia
• Tracheal Shifting
– LATE SIGN


Injuri Paru-Paru
• Hemothorax
– Accumulation of blood in the pleural space
– Serious hemorrhage may accumulate 1,500 mL of
blood
• Mortality rate of 75%
• Each side of thorax may hold up to 3,000 mL
– Blood loss in thorax causes a decrease in tidal
volume
• Ventilation/Perfusion Mismatch & Shock
– Typically accompanies pneumothorax
• Hemopneumothorax



Hemothorax sign & symptoms
• Blunt or penetrating chest trauma
• Shock
– Dyspnea
– Tachycardia
– Tachypnea
– Diaphoresis
– Hypotension
• Dull to percussion over injured side

Pulmonary Injury
• Pulmonary Contusion– Soft tissue contusion of the lung
– 30-75% of patients with significant blunt chest trauma
– Frequently associated with rib fracture
– Typical MOI• Deceleration
– Chest impact on steering wheel
• Bullet Cavitation– High velocity ammunition
– Microhemorrhage may account for 1- 1 ½ L of blood loss in alveolar tissue
• Progressive deterioration of ventilatory status
– Hemoptysis typically present

Cardiovascular injury
• Myocardial Contusion
– Occurs in 76% of patients with severe blunt chest trauma
– Right Atrium and Ventricle is commonly injured
– Injury may reduce strength of cardiac contractions
• Reduced cardiac output
– Electrical Disturbances due to irritability of damaged myocardial cells
– Progressive Problems
• Hematoma
• Hemopericard
• Myocardial necrosis
• Dysrhythmias
• CHF & or Cardiogenic shock

Myocardial contusion sign & symptom
• Bruising of chest wall
• Tachycardia and/or irregular rhythm
• Retrosternal pain similar to MI
• Associated injuries
– Rib/Sternal fractures
• Chest pain unrelieved by oxygen
– May be relieved with rest
– THIS IS TRAUMA-RELATED PAIN• Similar signs and symptoms of medical chest pain

Cardiovascular injury
• Pericardial Tamponade
– Restriction to cardiac filling caused by blood or other
fluid within the pericardium
– Occurs in <2% of all serious chest trauma
• However, very high mortality
– Results from tear in the coronary artery or penetration
of myocardium
• Blood seeps into pericardium and is unable to escape
• 200-300 ml of blood can restrict effectiveness of cardiac
contractions
– Removing as little as 20 ml can provide relief

Pericardial Tamponade Signs & Symptoms
• Dyspnea
• Possible cyanosis
• Beck’s Triad
– JVD
– Distant heart tones
– Hypotension or
narrowing pulse
pressure
• Weak, thready pulse
• Shock
• Kussmaul’s sign
– Decrease or absence of
JVD during inspiration
• Pulsus Paradoxus
– Drop in SBP >10 during
inspiration
– Due to increase in CO2
during inspiration
• Electrical Alterans
– P, QRS, & T amplitude
changes in every other
cardiac cycle
• PEA

Cardiovascular injury
• Traumatic Aneurysm or Aortic Rupture
– Aorta most commonly injured in severe blunt or penetrating trauma
• 85-95% mortality
– Typically patients will survive the initial injury insult
• 30% mortality in 6 hrs
• 50% mortality in 24 hrs
• 70% mortality in 1 week
– Injury may be confined to areas of aorta attachment
– Signs & Symptoms
• Rapid and deterioration of vitals
• Pulse deficit between right and left upper or lower extremities

Assessment of the Thoracic
Trauma Patient
• Scene Size-up
• Initial Assessment
• Rapid Trauma Assessment– Observe
• JVD, SQ Emphysema, Expansion of chest
– Palpate
– Auscultate
– Percuss
– Blunt Trauma Assessment
– Penetrating Trauma Assessment
• Ongoing Assessment

General Management of the Chest Injury Patient
• Ensure ABC’s– High flow O2 via NRB
– Intubate if indicated
– Consider overdrive ventilation• If tidal volume less than 6,000 mL
• BVM at a rate of 12-16– May be beneficial for chest contusion and rib fractures
– Promotes oxygen perfusion of alveoli and prevents atelectasis
• Anticipate Myocardial Compromise
• Shock Management– Fluid Bolus: 20 mL/kg
– AUSCULTATE! AUSCULATE! AUSCULATE!

Management of the Chest Injury
Patient
• Rib Fractures
– Consider analgesics for pain and to improve
chest excursion
• Morphine Sulfate
– CONTRAINDICATION
• Nitrous Oxide
– May migrate into pleural or mediastinal space and
worsen condition

Management of the Chest Injury
Patient• Sternoclavicular Dislocation
– Supportive O2 therapy
– Evaluate for concomitant injury
• Flail Chest
– Place patient on side of injury• ONLY if spinal injury is NOT suspected
– Expose injury site
– Dress with bulky bandage against flail segment• Stabilizes fracture site
– High flow O2
• Consider PPV or ET if decreasing respiratory status
– DO NOT USE SANDBAGS TO STABILIZE FX

Trauma.org

Management of the Chest Injury
Patient
• Open Pneumothorax
– High flow O2
– Cover site with sterile
occlusive dressing
taped on three sides
– Progressive airway
management if
indicated

Management of the Chest Injury
Patient• Tension Pneumothorax
– Confirmation
• Auscultaton & Percussion
– Pleural Decompression
• 2nd intercostal space in mid-clavicular line
– TOP OF RIB
• Consider multiple decompression sites if patient remains symptomatic
• Large over the needle catheter: 14ga

Management of the Chest Injury
Patient
• Hemothorax
– High flow O2
– 2 large bore IV’s• Maintain SBP of 90-100
• EVALUATE BREATH SOUNDS for fluid overload
• Myocardial Contusion
– Monitor ECG• Alert for dysrhythmias
– IV if antidysrhythmics are needed

Management of the Chest Injury
Patient
• Pericardial Tamponade– High flow O2
– IV therapy
– Consider pericardiocentesis; rapidly deteriorating patient
• Aortic Aneurysm– AVOID jarring or rough handling
– Initiate IV therapy enroute• Mild hypotension may be protective
• Rapid fluid bolus if aneurysm ruptures
– Keep patient calm

Diagnosa keperawatan
1. Ketidakefektifan pola pernapasan berhubungan dengan ekpansi paru yang tidak maksimal karena akumulasi udara/cairan.
2. Inefektif bersihan jalan napas berhubungan dengan peningkatan sekresi sekret dan penurunan batuk sekunder akibat nyeri dan keletihan.
3. Perubahan kenyamanan : Nyeri akut berhubungan dengan trauma jaringan dan reflek spasme otot sekunder.
4. Kerusakan integritas kulit berhubungan dengan trauma mekanik terpasang bullow drainage.
5. Hambatan mobilitas fisik berhubungan dengan ketidakcukupan kekuatan dan ketahanan untuk ambulasi dengan alat eksternal.
6. Risiko terhadap infeksi berhubungan dengan tempat masuknya organisme sekunder terhadap trauma.

Tujuan : Pola pernapasan efektive.
Kriteria hasil :
o Memperlihatkan frekuensi pernapasan yang efektive.
o Mengalami perbaikan pertukaran gas-gas pada paru.
o Adaptive mengatasi faktor-faktor penyebab.
Intervensi :
Berikan posisi yang nyaman, biasanya dnegan peninggian kepala tempat
tidur. Balik ke sisi yang sakit. Dorong klien untuk duduk sebanyak mungkin.
Observasi fungsi pernapasan, catat frekuensi pernapasan, dispnea atau
perubahan tanda-tanda vital.
Jelaskan pada klien bahwa tindakan tersebut dilakukan untuk menjamin
keamanan
Ketidakefektifan pola pernapasan berhubungan dengan ekspansi paru
yang tidak maksimal karena trauma.

Intervensi …
• Jelaskan pada klien tentang etiologi/faktor pencetus adanya sesak atau kolaps paru-paru.
• Pertahankan perilaku tenang, bantu pasien untuk kontrol diri dnegan menggunakan pernapasan lebih lambat dan dalam.
• Perhatikan alat chest drainase berfungsi baik, cek setiap 1 – 2 jam
• Periksa pengontrol penghisap untuk jumlah hisapan yang benar.
• Periksa batas cairan pada botol penghisap, pertahankan pada batas yang ditentukan.
• Observasi gelembung udara botol penampung.
• Posisikan sistem drainage slang untuk fungsi optimal, yakinkan slang tidak terlipat, atau menggantung di bawah saluran masuknya ke tempat drainage. Alirkan akumulasi drainase bila perlu.
• Catat karakter/jumlah drainage selang dada.
• Kolaborasi dengan tim kesehatan lain Pemberian analgetika. Konsul photo toraks.

Inefektif bersihan jalan napas berhubungan dengan peningkatan sekresi
sekret dan penurunan batuk sekunder akibat nyeri dan keletihan.
Tujuan : Jalan napas lancar/normalKriteria hasil :• Menunjukkan batuk yang efektif.• Tidak ada lagi penumpukan sekret di sal. pernapasan.• Klien nyaman.
Intervensi :• Jelaskan klien tentang kegunaan batuk yang efektif dan mengapa
terdapat penumpukan sekret di saluran pernapasan.
• Ajarkan latihan pernapasan dan batuk efektif
• Auskultasi paru sebelum dan sesudah klien batuk.
• Ajarkan mempertahankan hidrasi yang adekuat; meningkatkan masukan cairan 1000 sampai 1500 cc/hari bila tidak kontraindikasi.
• Dorong atau berikan perawatan mulut yang baik setelah batuk.
• Lakukan penghisapan lendir jika diperlukan
• Kolaborasi dengan tim kesehatan lain : Pemberian expectoran, pemberian analgesik,