
Drug Resistance Tuberculosis - moh.gov.myhsibu.moh.gov.my/hsb.bm/artikel/kursusTB/Drug Resistant...
55
Drug Resistance Tuberculosis Dr Tie Siew Teck Respiratory Physician SGH
Transcript of Drug Resistance Tuberculosis - moh.gov.myhsibu.moh.gov.my/hsb.bm/artikel/kursusTB/Drug Resistant...
Drug Resistance Tuberculosis
Dr Tie Siew TeckRespiratory Physician
SGH
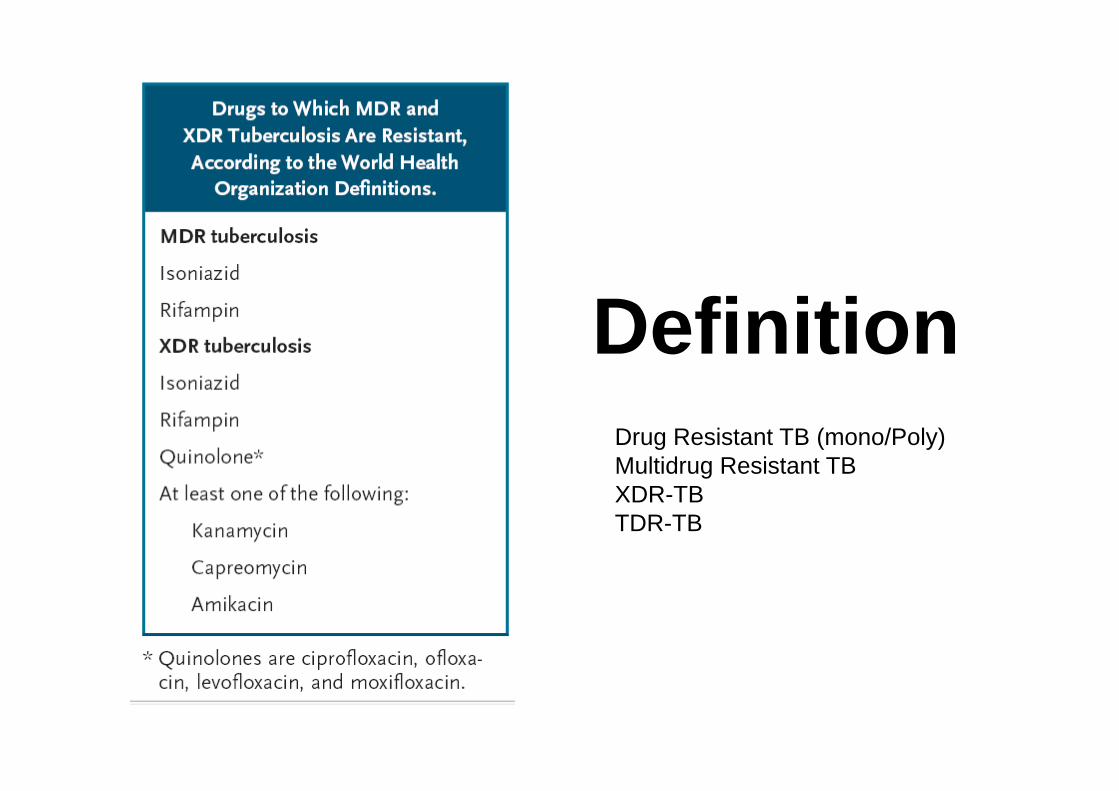
DefinitionDrug Resistant TB (mono/Poly)Multidrug Resistant TBXDR-TBTDR-TB
Burden of DRTB
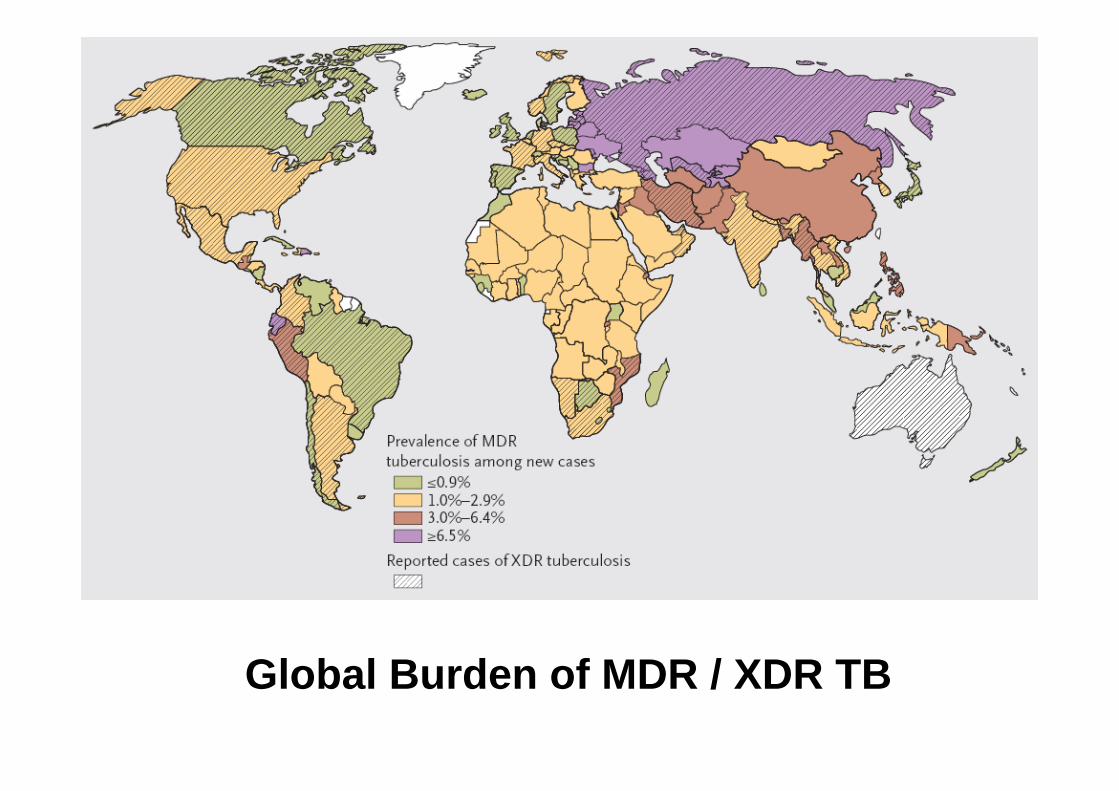
Global Burden of MDR / XDR TB
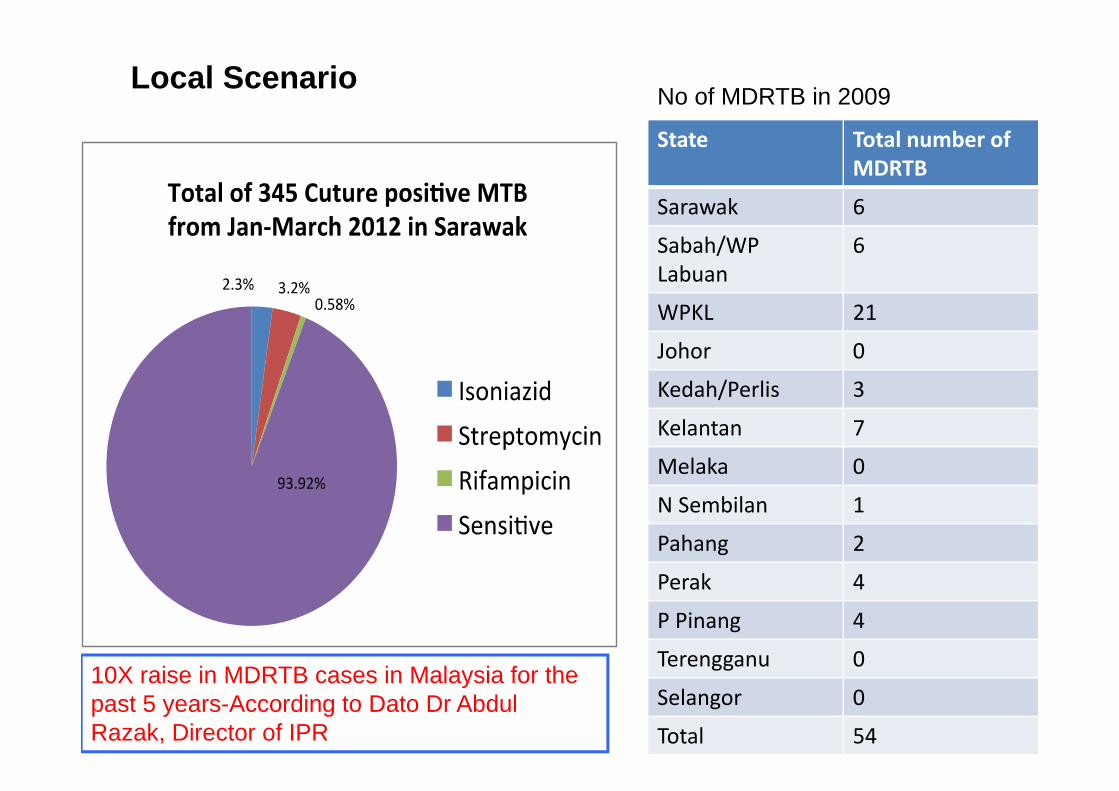
State Total number of MDRTB
Sarawak 6
Sabah/WP Labuan
6
WPKL 21
Johor 0
Kedah/Perlis 3
Kelantan 7
Melaka 0
N Sembilan 1
Pahang 2
Perak 4
P Pinang 4
Terengganu 0
Selangor 0
Total 54
No of MDRTB in 2009Local Scenario
10X raise in MDRTB cases in Malaysia for the past 5 years-According to Dato Dr Abdul Razak, Director of IPR
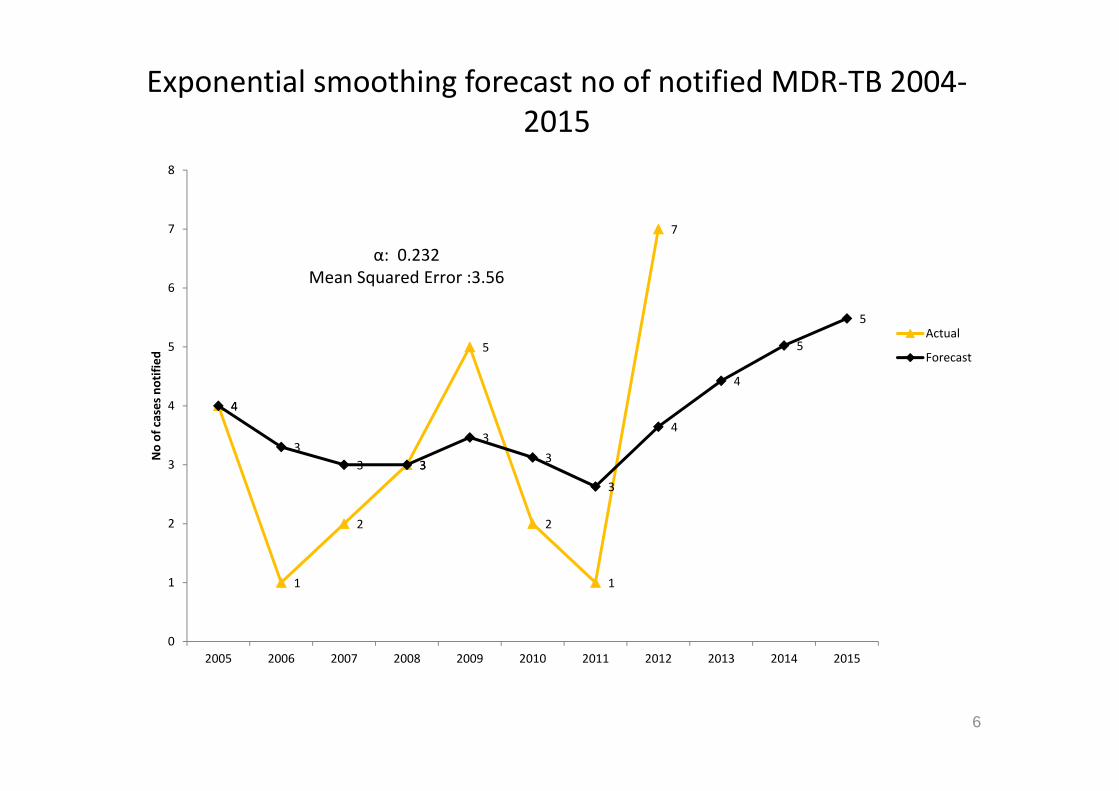
Exponential smoothing forecast no of notified MDR‐TB 2004‐2015
4
1
2
3
5
2
1
7
4
33 3
33
3
4
4
5
5
0
1
2
3
4
5
6
7
8
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
No of cases notified
Actual
Forecast
α: 0.232Mean Squared Error :3.56
6
Evolution and Genetic basis of Drug‐Resistant TB
Evolution and Genetic basis of Drug‐Resistant TB
• Epidemiological classification of drug resistance in TB:
1. Primary drug resistance: when previously untreated patients are found to have drug‐resistant organisms, presumably because they have been infected from an outside source of resistant bacteria.
2. Acquired drug resistance: when patients who initially have drug‐susceptible TB bacteria later become drug‐resistant as a result of inadequate, inappropriate or irregular treatment or, nonadherence in drug taking.
3. Initial drug resistance: when drug resistance occurs in patients who deny previous treatment but whose drug use history cannot be verified.
Why this problem arise?• MDRTB is entirely MAN MADE.• Sloppy implementation of DOTS.• Monotherapy
– Eg INH resistance. • Wrong antiTB dosage.• Poor compliance to ATT. • HIV
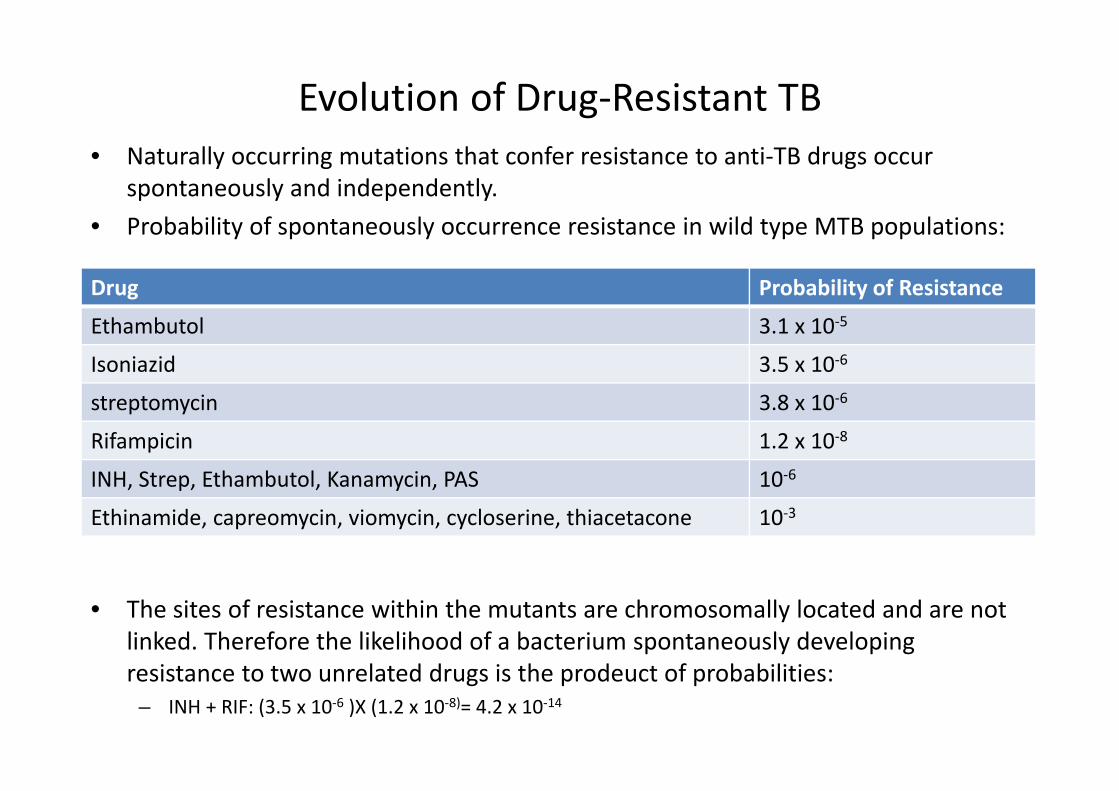
Evolution of Drug‐Resistant TB• Naturally occurring mutations that confer resistance to anti‐TB drugs occur
spontaneously and independently. • Probability of spontaneously occurrence resistance in wild type MTB populations:
• The sites of resistance within the mutants are chromosomally located and are not linked. Therefore the likelihood of a bacterium spontaneously developing resistance to two unrelated drugs is the prodeuct of probabilities:
– INH + RIF: (3.5 x 10‐6 )X (1.2 x 10‐8)= 4.2 x 10‐14
Drug Probability of Resistance
Ethambutol 3.1 x 10‐5
Isoniazid 3.5 x 10‐6
streptomycin 3.8 x 10‐6
Rifampicin 1.2 x 10‐8
INH, Strep, Ethambutol, Kanamycin, PAS 10‐6
Ethinamide, capreomycin, viomycin, cycloserine, thiacetacone 10‐3
Evolution of Drug‐Resistant TB
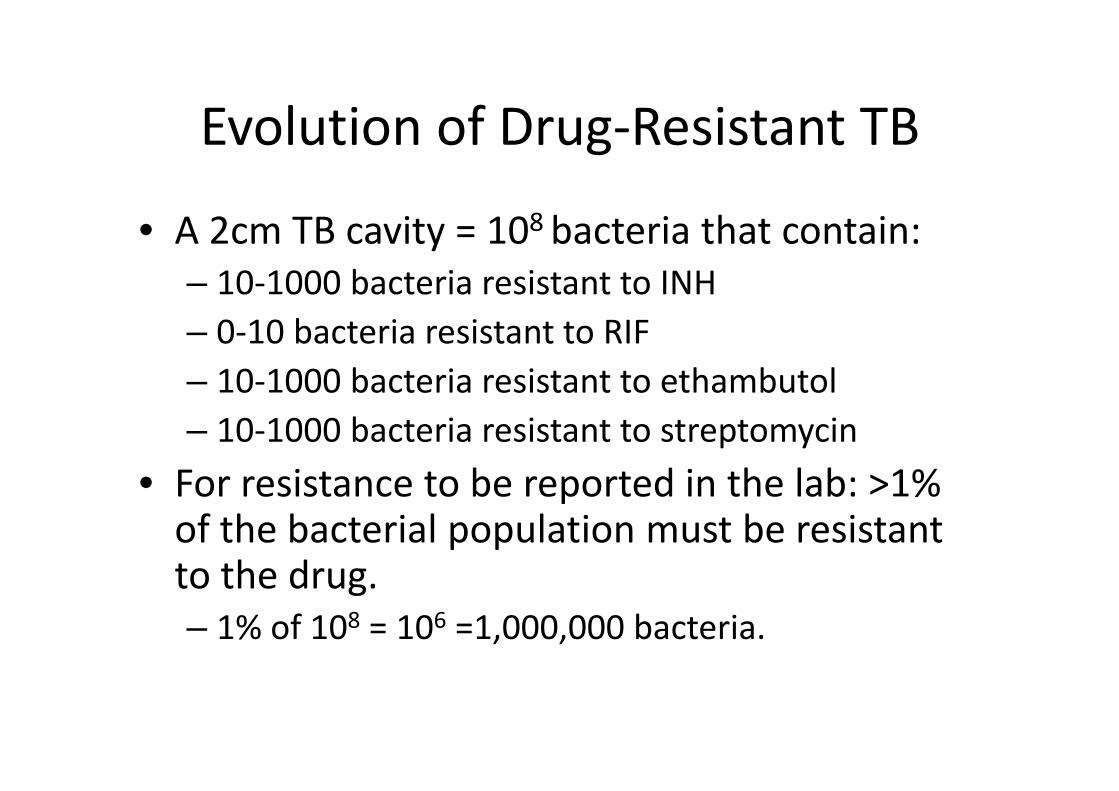
• A 2cm TB cavity = 108 bacteria that contain: – 10‐1000 bacteria resistant to INH– 0‐10 bacteria resistant to RIF– 10‐1000 bacteria resistant to ethambutol– 10‐1000 bacteria resistant to streptomycin
• For resistance to be reported in the lab: >1% of the bacterial population must be resistant to the drug. – 1% of 108 = 106 =1,000,000 bacteria.
Evolution of Drug‐Resistant TB
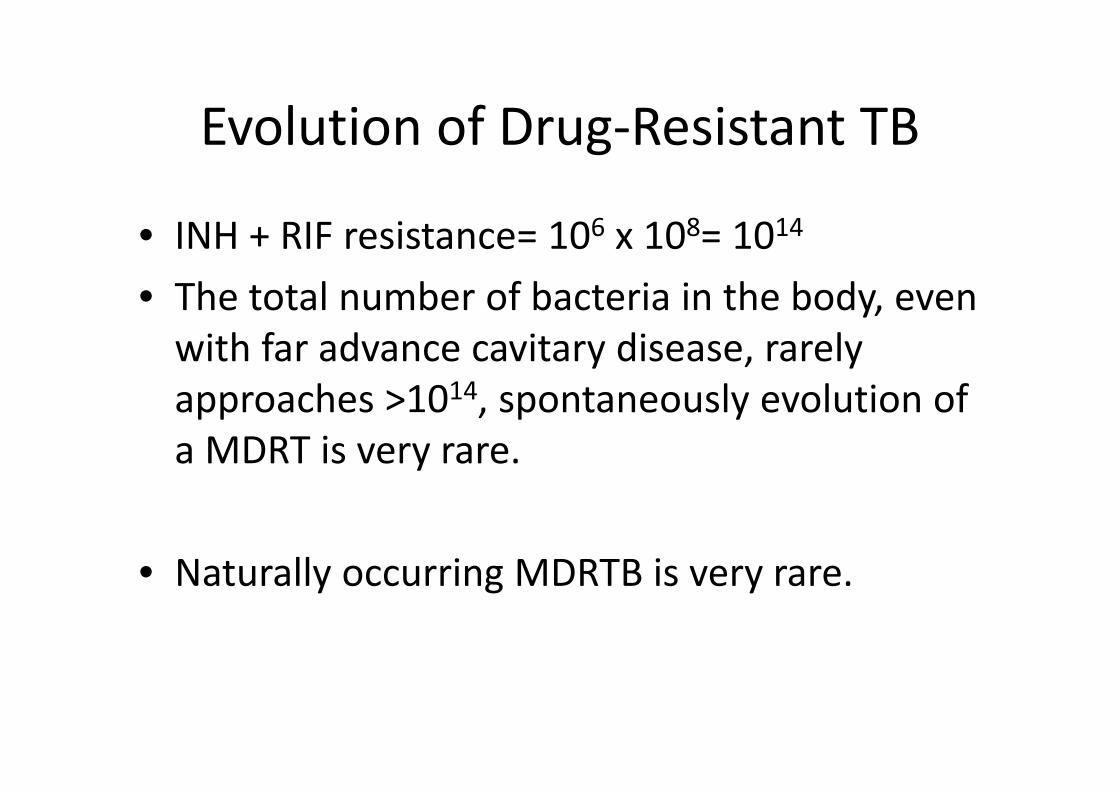
• INH + RIF resistance= 106 x 108= 1014
• The total number of bacteria in the body, even with far advance cavitary disease, rarely approaches >1014, spontaneously evolution of a MDRT is very rare.
• Naturally occurring MDRTB is very rare.
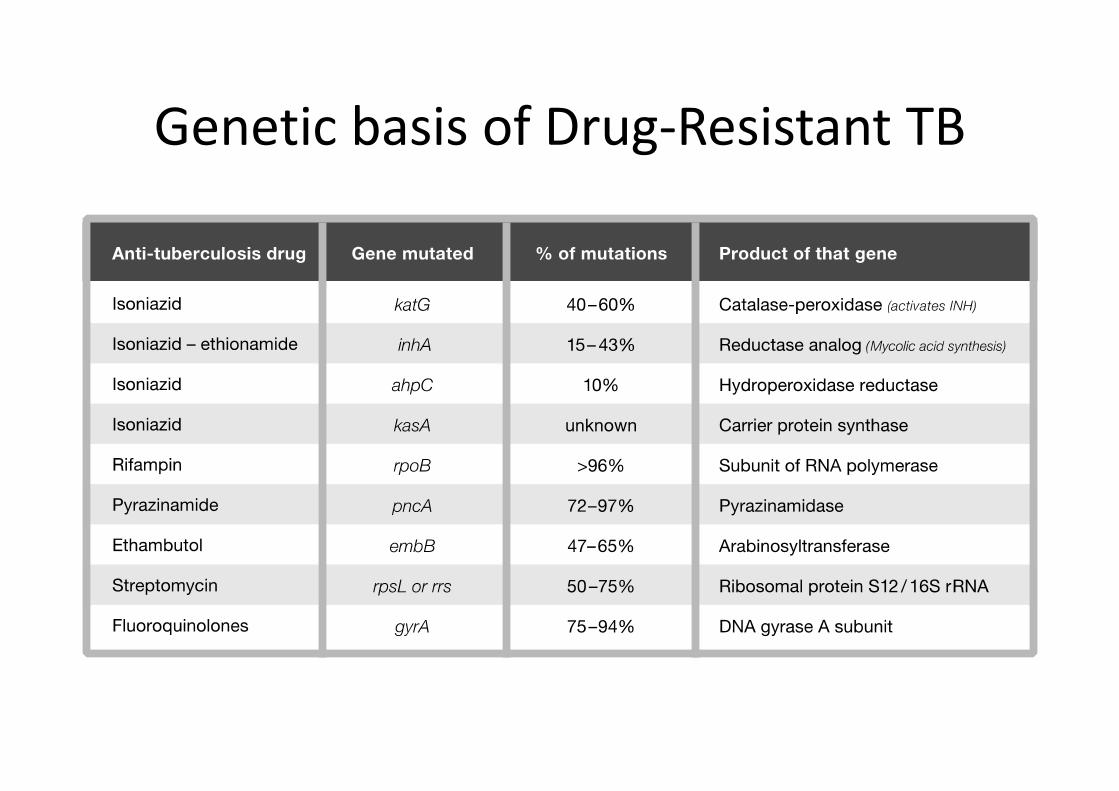
Genetic basis of Drug‐Resistant TB
Clinical Predictors of DRTB
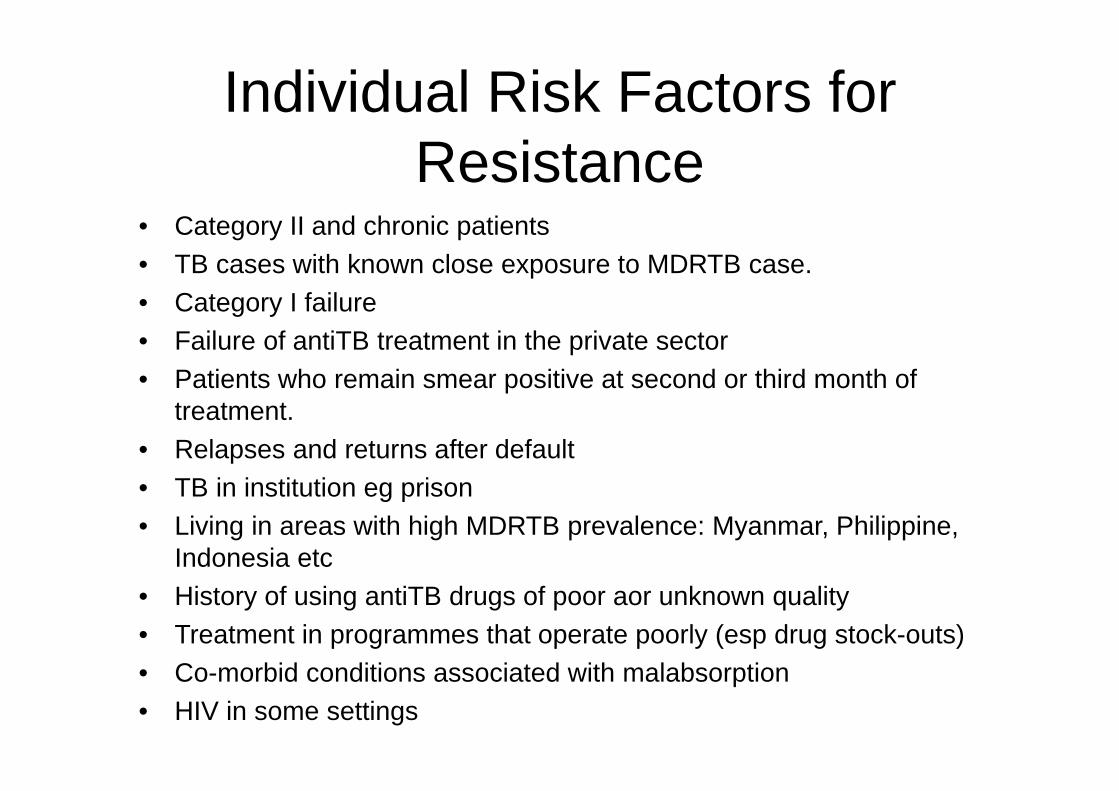
Individual Risk Factors for Resistance
• Category II and chronic patients• TB cases with known close exposure to MDRTB case.• Category I failure• Failure of antiTB treatment in the private sector• Patients who remain smear positive at second or third month of
treatment. • Relapses and returns after default• TB in institution eg prison• Living in areas with high MDRTB prevalence: Myanmar, Philippine,
Indonesia etc• History of using antiTB drugs of poor aor unknown quality• Treatment in programmes that operate poorly (esp drug stock-outs)• Co-morbid conditions associated with malabsorption• HIV in some settings
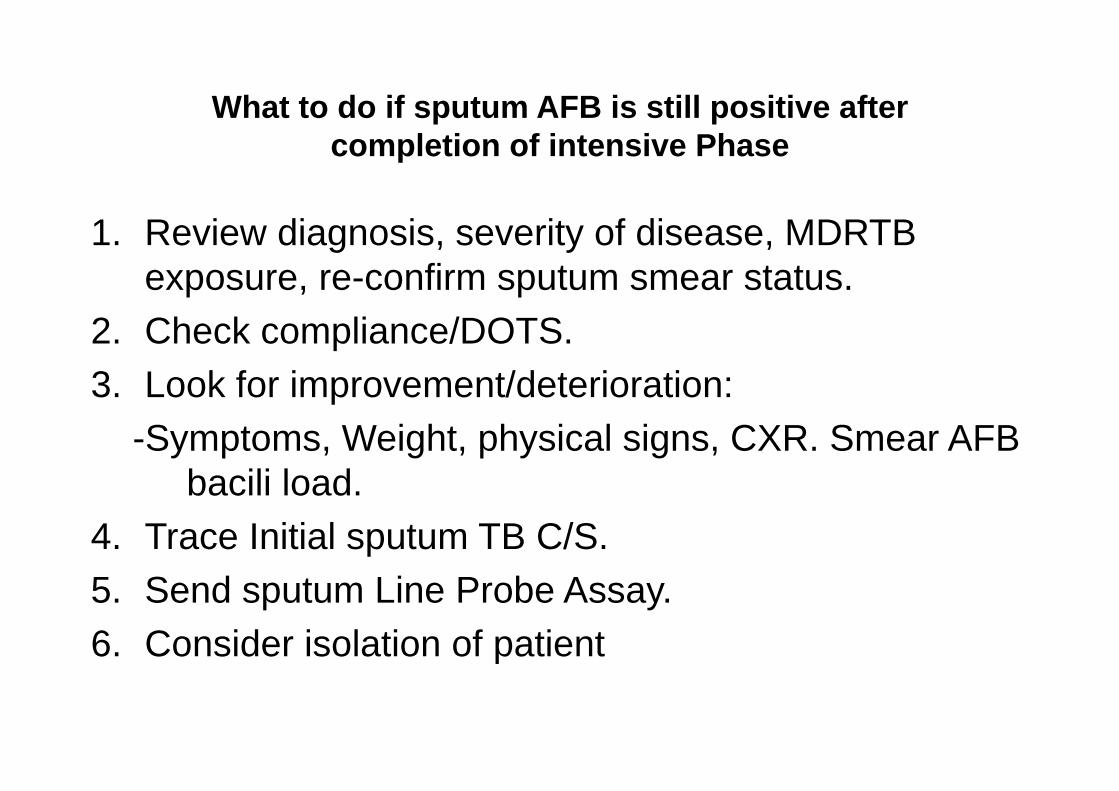
What to do if sputum AFB is still positive after completion of intensive Phase
1. Review diagnosis, severity of disease, MDRTB exposure, re-confirm sputum smear status.
2. Check compliance/DOTS. 3. Look for improvement/deterioration:
-Symptoms, Weight, physical signs, CXR. Smear AFB bacili load.
4. Trace Initial sputum TB C/S. 5. Send sputum Line Probe Assay.6. Consider isolation of patient.
What to do if sputum AFB is still positive after completion of intensive Phase
• Refer to physician for advise. • Possible explanations:
– Dead bacilli– Delayed smear conversion– Superimposed NTM– Drug resistance – Wrong report.
• Consider to prolonged intensive phase (IF DRUG RESISTNACE SUSPECTED) or prolonged maintenance phase (NO RESISTANCE, HIGH BACILLARY LOAD)
MDRTB CAN+SHOULD only be diagnosed by TB Culture and Sensitivity.
• Phenotypic DST• Genotypic DST
Conventional phenotypic Susceptibility Methods
1. Proportional method2. Absolute concentration method3. Resistance ratio method
• Need at least 2‐3 months. • Inter‐laboratory variability.• Still the gold standard.
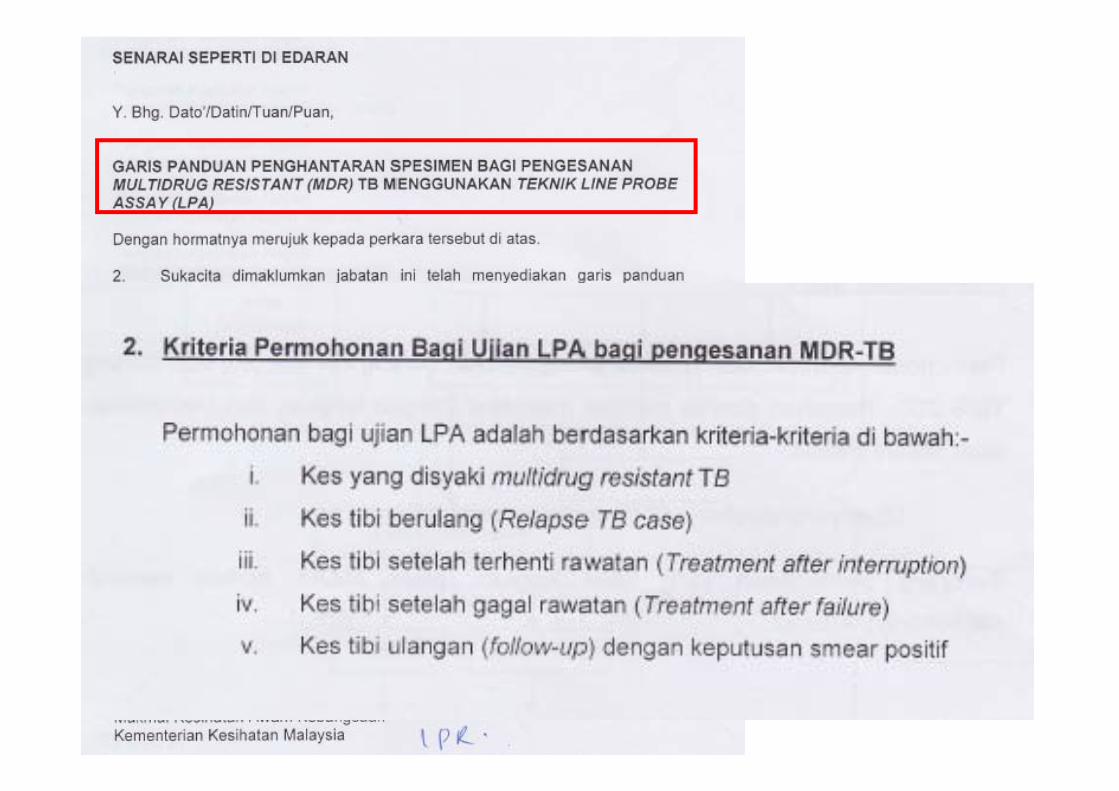
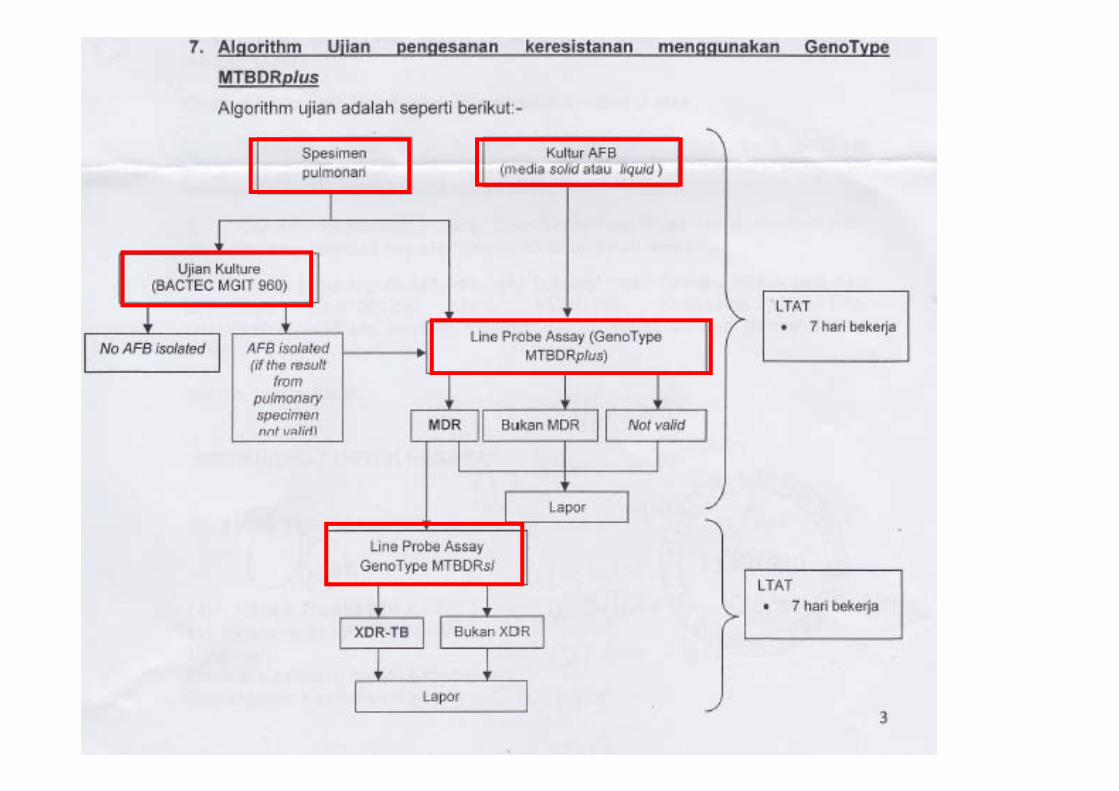
Genotypic Resistance Testing: Line Probe Assay
• Endorsed by WHO in 2008 for molecular detection of drug resistance from smear positive patients at risk of MDRTB.
• 2 commercial tests available:– GenoType MTBDRplus Test (Hain Lifescience)– INNO-LiPA Rif.TB Test (Innogenetics NV)
• Sensitivity>97% and specificity>99% for RIF resistance.• Sensitivity 84% and specificity>99% for INH resistance. • Can be done of specimen vs isolate.• Result in 5H. (7days in Malaysia)
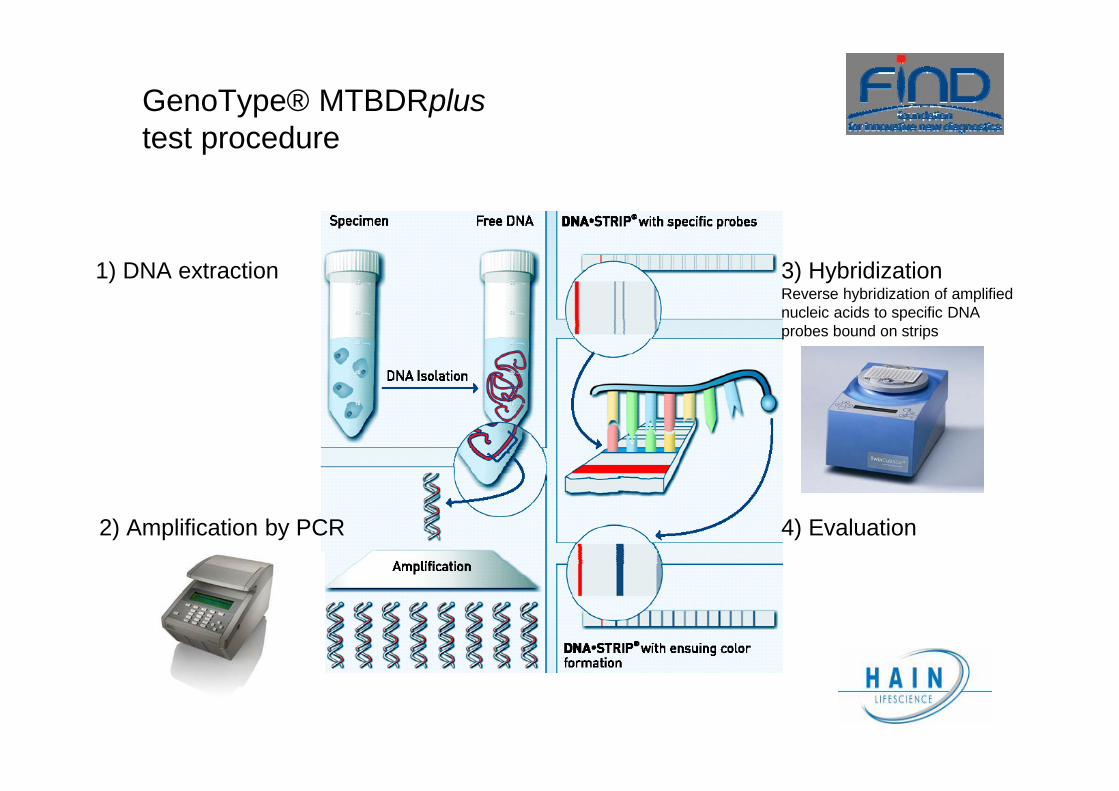
GenoType® MTBDRplustest procedure
1) DNA extraction
2) Amplification by PCR
3) HybridizationReverse hybridization of amplifiednucleic acids to specific DNAprobes bound on strips
4) Evaluation
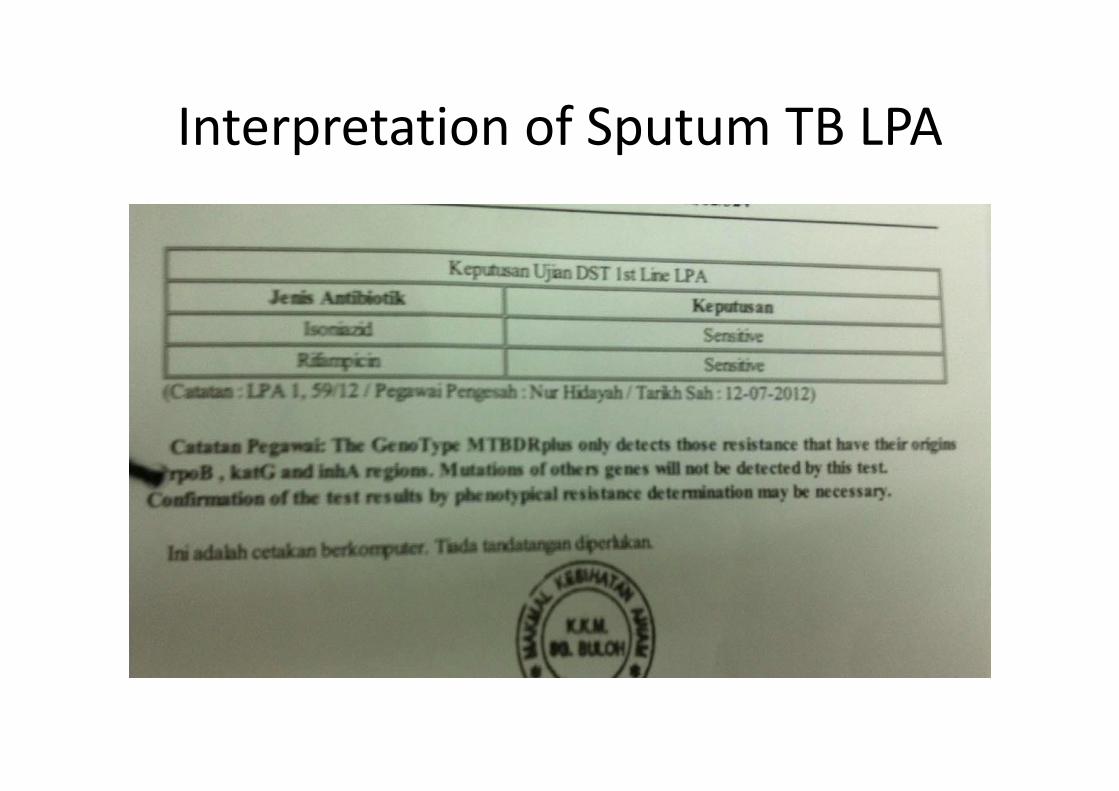
Interpretation of Sputum TB LPA
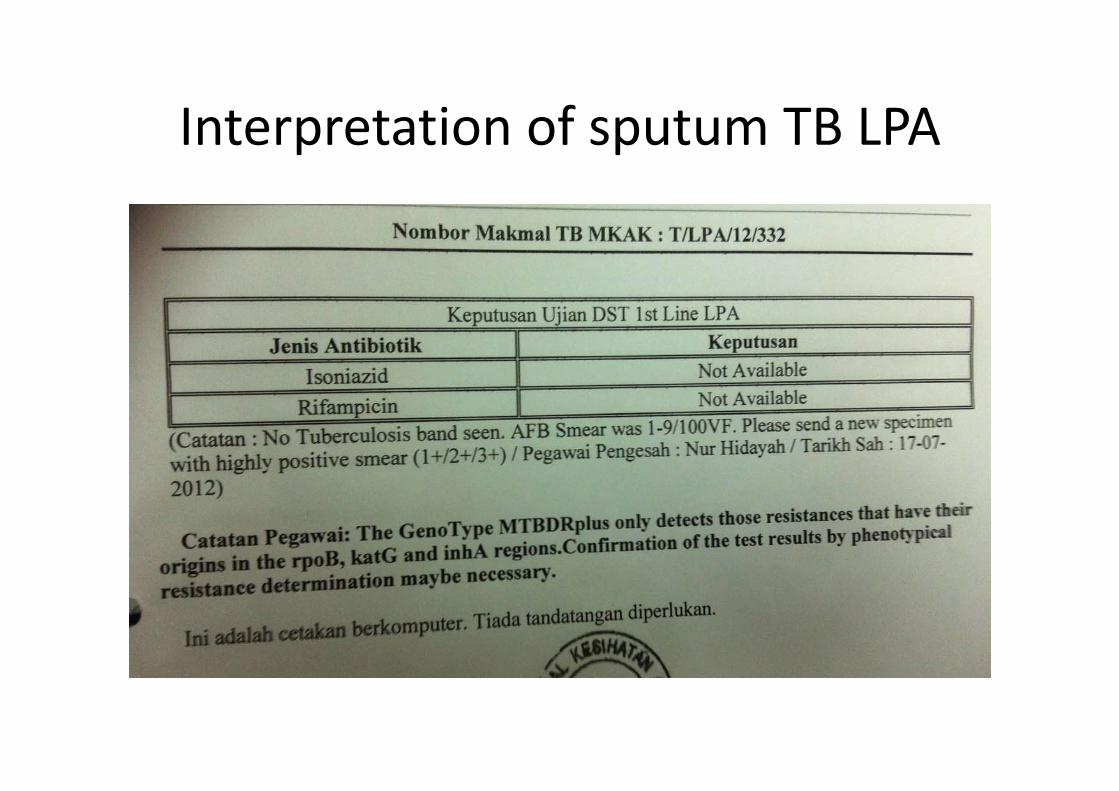
Interpretation of sputum TB LPA
Management of DRTB
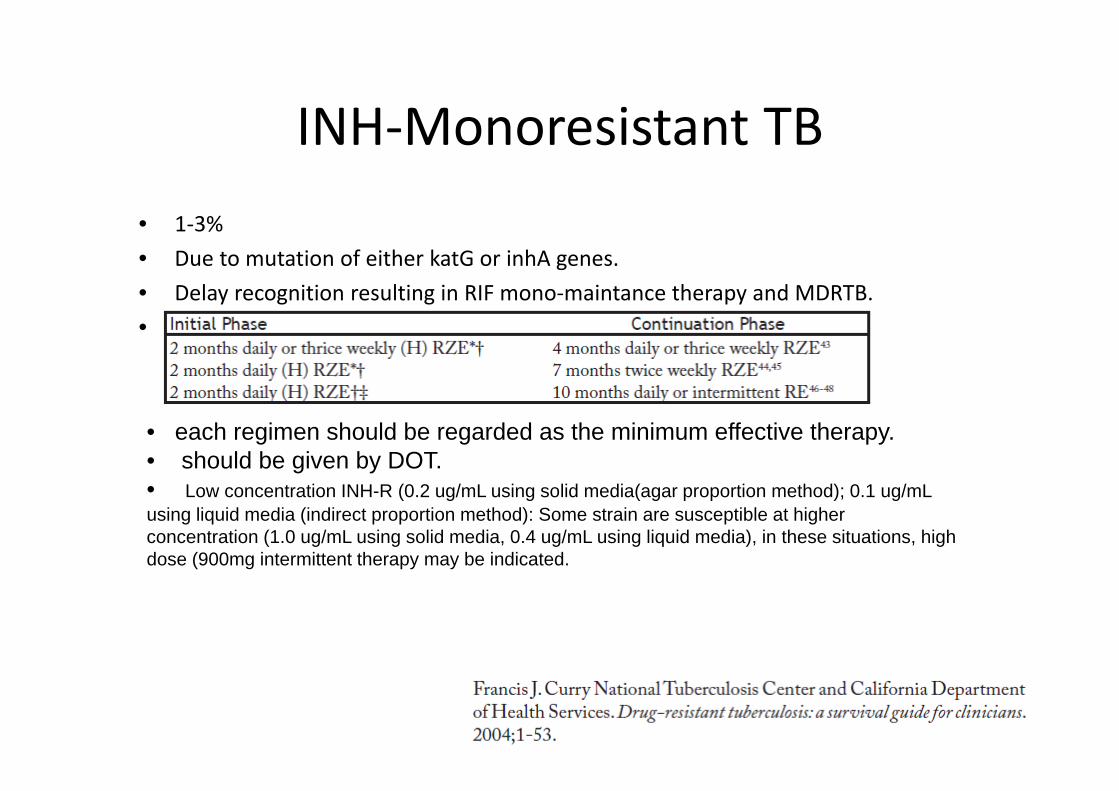
INH‐Monoresistant TB• 1‐3%• Due to mutation of either katG or inhA genes.• Delay recognition resulting in RIF mono‐maintance therapy and MDRTB.• Regimens proven to cure INH‐resistant TB:
• each regimen should be regarded as the minimum effective therapy.• should be given by DOT.• Low concentration INH-R (0.2 ug/mL using solid media(agar proportion method); 0.1 ug/mL using liquid media (indirect proportion method): Some strain are susceptible at higher concentration (1.0 ug/mL using solid media, 0.4 ug/mL using liquid media), in these situations, high dose (900mg intermittent therapy may be indicated.
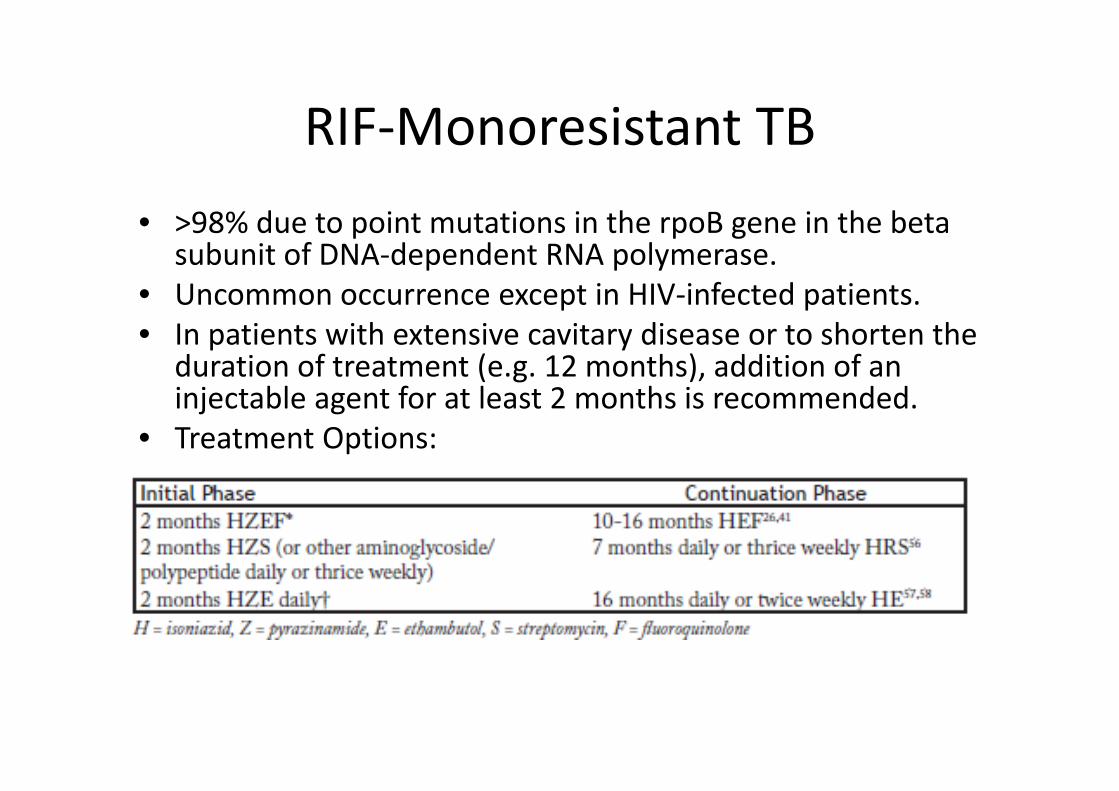
RIF‐Monoresistant TB• >98% due to point mutations in the rpoB gene in the beta
subunit of DNA‐dependent RNA polymerase. • Uncommon occurrence except in HIV‐infected patients. • In patients with extensive cavitary disease or to shorten the
duration of treatment (e.g. 12 months), addition of an injectable agent for at least 2 months is recommended.
• Treatment Options:
Mono‐resistance to PZA or Ethambutol
• PZA‐monoresistant TB is rare. • Occurs genotypiccally in M. bovis.• Treatment regimen: 2(HER) 7 (HR)
• Ethambutol monoresistance will not change the efficacacy or duration of treatment with standard regimens.
• 2(HRZ) 4(HR)
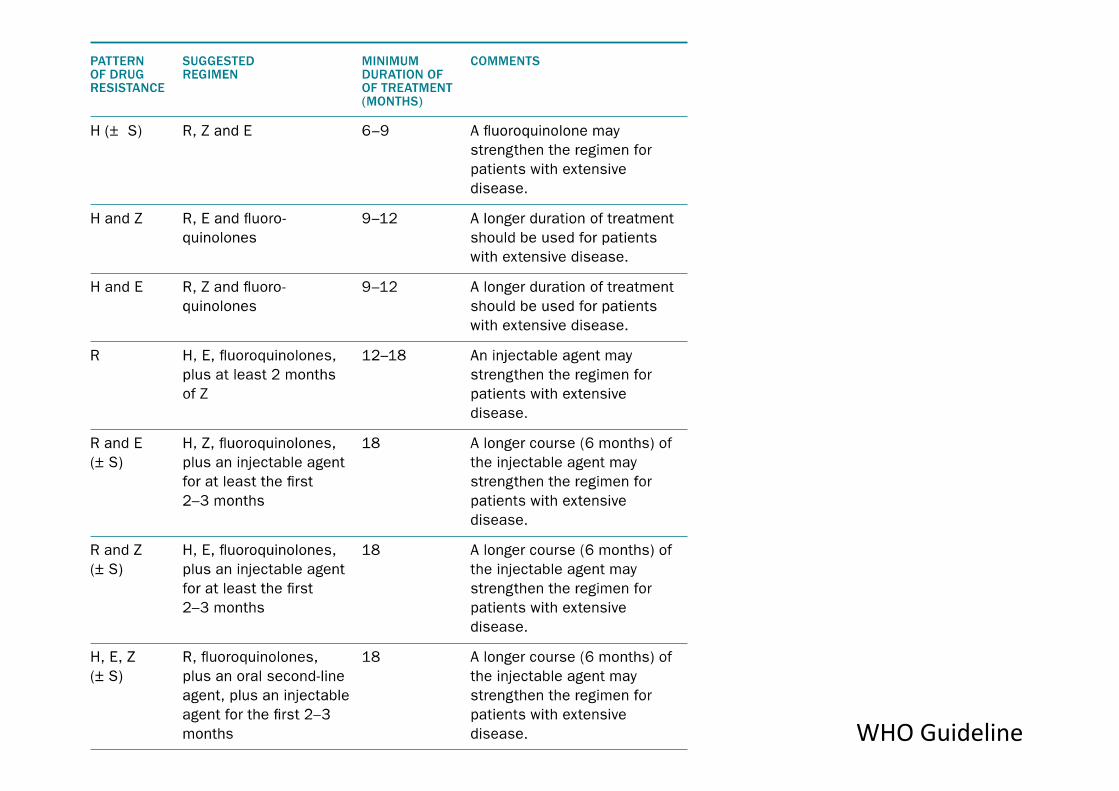
WHO Guideline
MDRTB• Resistant to at least RIF + INH• The strongest determinant of MDRTB is previous treatment.
• Rifampicin resistance is a marker for MDRTB in >90% of cases.1
1. Dronbniewski FA et al. Molecular diagnosis, detection of drug resistance and epidemiology of tuberculosis. Br J Hosp Med 1996;56:204-208.
GENERAL PRINCIPALS IN MDRTB TREATMENT
PRINCIPAL 1: USE AT LEAST 4 DRUGS CERTAIN OR HIGHLY LIKELY TO BE EFFECTIVE
NEVER ADD ONE DRUG TO A FAILING REGIMEN
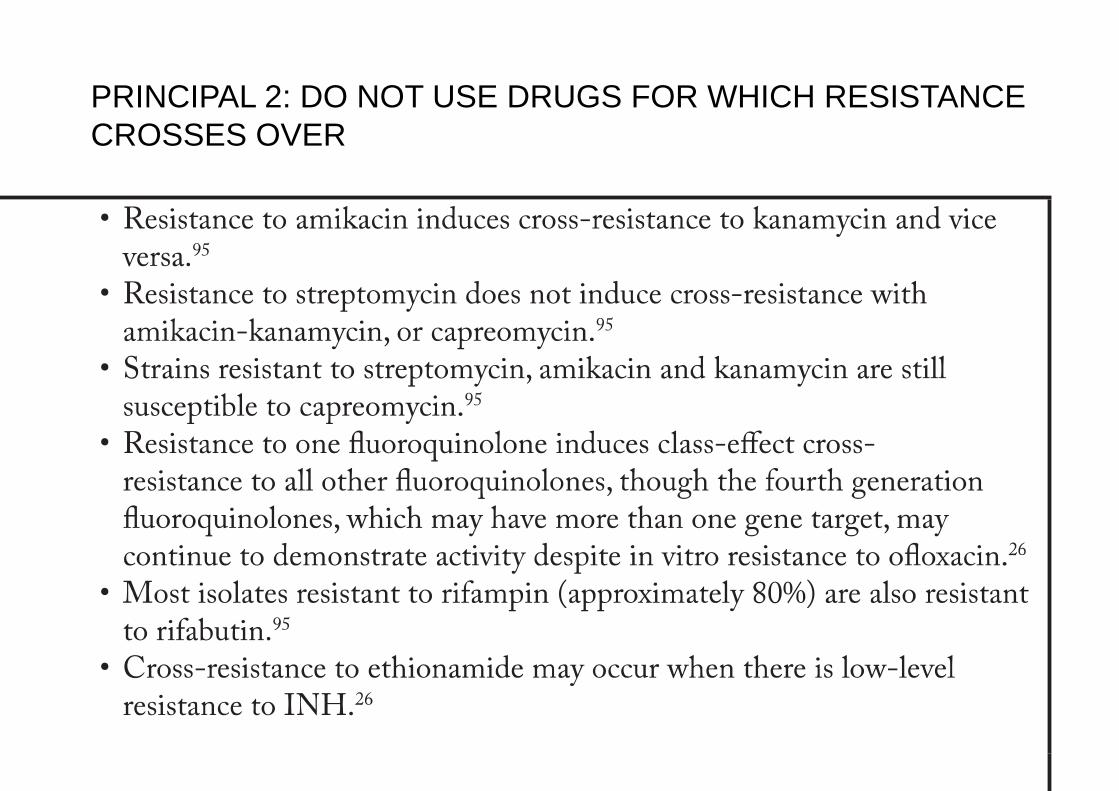
PRINCIPAL 2: DO NOT USE DRUGS FOR WHICH RESISTANCE CROSSES OVER
PRINCIPAL 3: ELIMINATE DRUGS THAT ARE NOT SAFE IN THE PATIENT
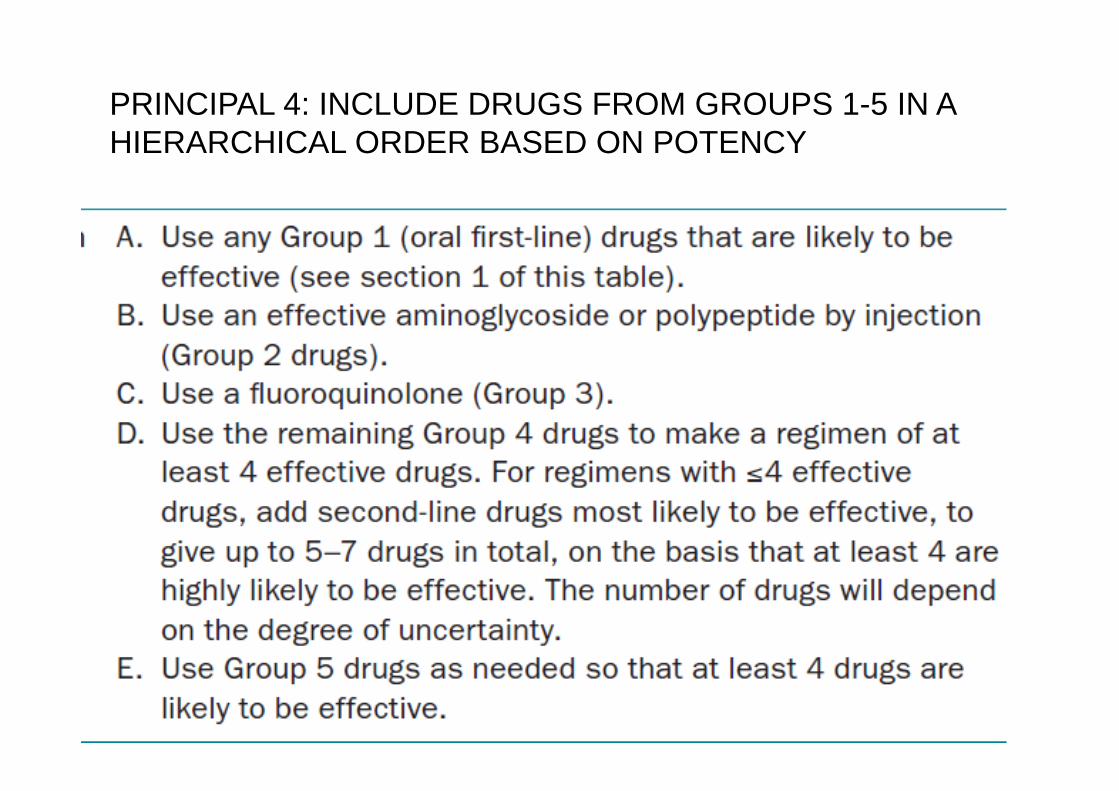
PRINCIPAL 4: INCLUDE DRUGS FROM GROUPS 1-5 IN A HIERARCHICAL ORDER BASED ON POTENCY

PRINCIPALS 5: BE PREPARED TO PREVENT, MONITOR AND MANAGE ADVERSE EFFECTS FRO EACH OF THE DRUGS SELECTED
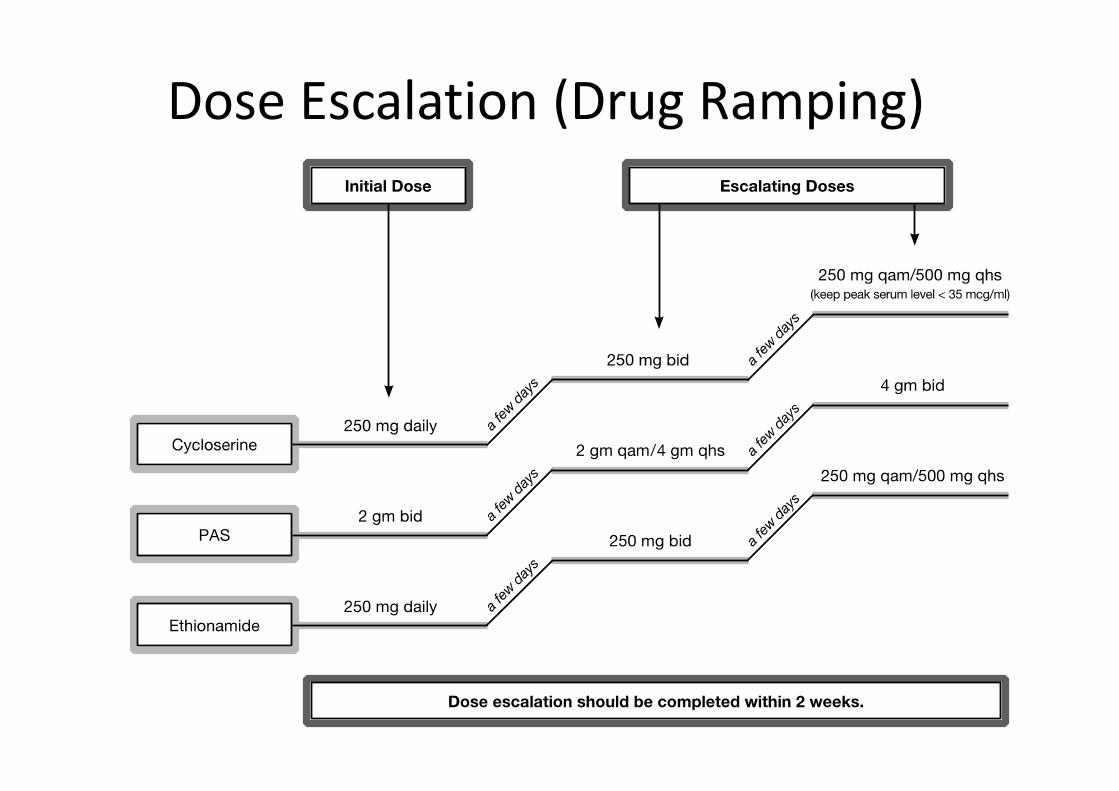
Dose Escalation (Drug Ramping)
Patient and DOT supervisor Counseling
• From the outset it should be made clear to patients, families, and staff that meticulous adherence to the prescribed regimen is critical to cure.
• Patient should try to tolerate any unpleasant side effects in order to achieve cure, agree to remain under direct observation with each dose supervised.
• BOTH THE PATIENT AND THE TREATEMENT CENTER MUST BE COMMITED IN MDRTB TREATMENT.

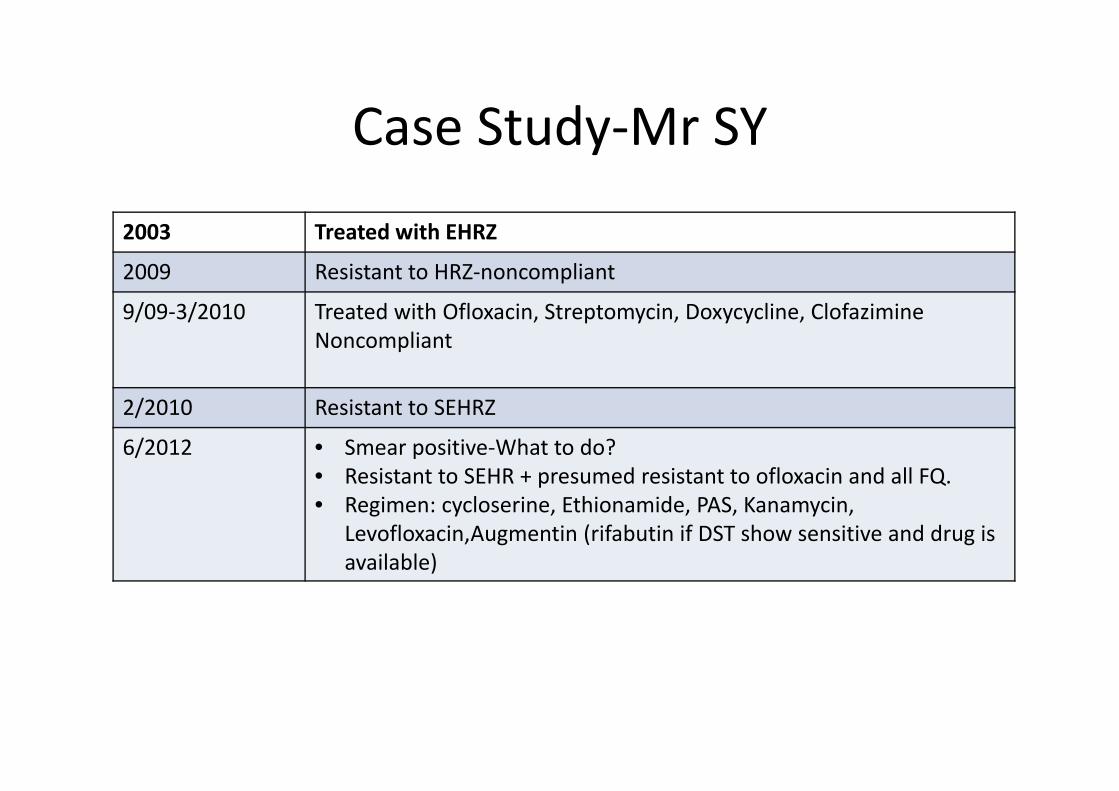
Case Study‐Mr SY
2003 Treated with EHRZ
2009 Resistant to HRZ‐noncompliant
9/09‐3/2010 Treated with Ofloxacin, Streptomycin, Doxycycline, ClofazimineNoncompliant
2/2010 Resistant to SEHRZ
6/2012 • Smear positive‐What to do?• Resistant to SEHR + presumed resistant to ofloxacin and all FQ.• Regimen: cycloserine, Ethionamide, PAS, Kanamycin,
Levofloxacin,Augmentin (rifabutin if DST show sensitive and drug is available)
Duration of MDRTB treatment
• 18 Months after culture conversion.• 6 months of injectable drug. Or extension
of 3 month after culture conversion
Outcome definition in MDRTB treatment
•Cure: completed treatment + has at least 5 consecutive negative cultures from samples collected at least 30 days apart in the final 12 months of treatment. (WHO)
Outcome of MDRTB Treatment
• Cure: 50‐70%, Mortality: 30%, • Best outcome: 70‐80% of cure.
– Absence of previous treatment– Use of FQ – Resistance to fewer drugs at the outset– HIV seronegativity
• Poor outcome:– History of previous MDRTB treatment– FQ resistance– Low BMI (<18.5)
Hospitalization of MDRTB Patients
• Initial hospitalization: – To achieve rapid control of the infection.– Securing the patient’s future cooperation.– Drugs ramping to enhance tolerance– Highly infectious patients.– Effective home isolation cannot be provided.
• Hospitalization during treatment– Side effects– Co‐morbidity
Surgery for MDRTB
• Selected on a case by case basis.• The goal of surgery is to remove as much as disease lungs as
possible, especially cavities.• Potential candidate:
– DST pattern that predict a high probability of treatment failure
– Disease sufficiently localised to permit resection of the bulk of involved lung with enough remaining functioning lung to prevent crippling respiratory impairement.
• Timing: ?3‐4 months of therapy and eradication of bacteria from the sputum.
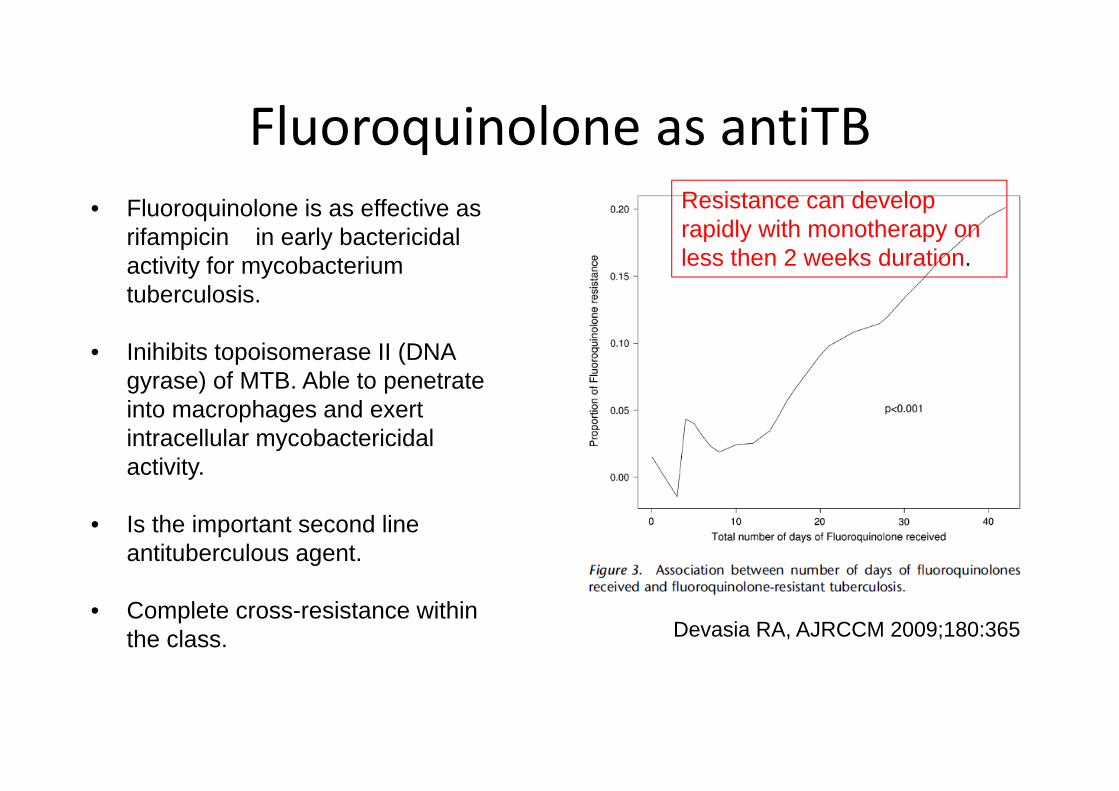
Fluoroquinolone as antiTB• Fluoroquinolone is as effective as
rifampicin in early bactericidal activity for mycobacterium tuberculosis.
• Inihibits topoisomerase II (DNA gyrase) of MTB. Able to penetrate into macrophages and exert intracellular mycobactericidal activity.
• Is the important second line antituberculous agent.
• Complete cross-resistance within the class. Devasia RA, AJRCCM 2009;180:365
Resistance can develop rapidly with monotherapy on less then 2 weeks duration.
THANK YOU
Isoniazid Resistance• 50% of resistance isolates contain mutations in katG.• 20‐34% of resistance isolates contain mutations in the promoter region of
inhA. Rarely in the coding region of inhA.– Most isolates that contain inhA mutations in the absence of mutations in katG
have relatively low level isoniazid resistance, < to 1Ug/mL. – Isolates with a complete deletion of katG can have MICs as high as 50Ug/mL.
• 10% of resistance isolate contain mutation in the ahpC promoter region.• Mutations in codons 66, 269, 312 and 413 of kasA were found in about
10% of resistance isolate.• ndhA, dfrA. • 10‐25% of INH‐resistant strains do not contain mutations in known gene
targets for isoniazid resistance. • The prevalence of mutations in the inhA and katG genes seems to vary
widely in different geographical locations. (1)
1. Barnard M et al. Rapid molecular screeening for multidrug-resistant tuberculosis in a high-volume public health laboratory in South Africa. AJRCCM2008:177:787.
The Paradox of Global TB Emergency
• WHO announced TB as global health emergency in 1997.
• We are in the state of TB Epidemic. • MTB discovered by Robert Koch in 1882, 24th March.
• 1/3 of world population is infected by TB. • World Bank estimated to cure TB using DOTS only needs 3/person/life saved.
• In all TB studies: Cure>95%
• Only ½ of all TB cases detected (WHO). • Only 65% cured(WHO). • Every year Globally 1.8 Millions people die of TB. • TB mortality is the highest infectious disease mortality in Malaysia
• WHY???
The Paradox of Global TB Emergency
WHO has designated 24th March of each year as world TB day. To mark the anniversary of Robert Koch’s discovery. This is not a day for celebration, instead it is one of which the global community should reflect on the tragic failure of our system on TB control. The ignorant, complaisant attitude towards TB Control.
Prof Alimnudin Zumla, Imperial College, Lancet 1999.


















