N SUCI W RHEUMATOID ARTHRITIS.pdf
39
BIODATA • • Nama : dr. Nyoman Suci Widyastiti, M.Kes, SpPK • Riwayat pendidikan : - Dokter Umum FK UNDIP, 1996 - Magister Biomedik konsentrasi Imunologi, Program Pasca Sarjana UNDIP, 2000 - Spesialis Patologi Klinik FK UNDIP, 2005 - S3 Kedokteran Unair, 2008 – sekarang Riwayat pekerjaan : - Staf Pengajar Bagian Patologi Klinik FK UNDIP 1996- sekarang - Staf pengajar Pasca Sarjana / S2 Biomedik UNDIP 2001 – sekarang - Sekretaris Program Studi PPDS Patologi Klinik UNDIP 2009- sekarang
-
Upload
jamaluddin-ahmad-am -
Category
Documents
-
view
243 -
download
3
Transcript of N SUCI W RHEUMATOID ARTHRITIS.pdf
-
BIODATA
Nama : dr. Nyoman Suci Widyastiti, M.Kes, SpPK Riwayat pendidikan : - Dokter Umum FK UNDIP, 1996 - Magister Biomedik konsentrasi Imunologi, Program Pasca Sarjana UNDIP, 2000 - Spesialis Patologi Klinik FK UNDIP, 2005 - S3 Kedokteran Unair, 2008 sekarang Riwayat pekerjaan : - Staf Pengajar Bagian Patologi Klinik FK UNDIP 1996- sekarang - Staf pengajar Pasca Sarjana / S2 Biomedik UNDIP 2001 sekarang - Sekretaris Program Studi PPDS Patologi Klinik UNDIP 2009- sekarang
-
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS FROM BASIC TO CLINICFROM BASIC TO CLINIC
Nyoman Suci WBagian Patologi Klinik
FK UNDIP/RS dr Kariadi
-
One of the most common systemic autoimmune diseases, affecting approximately 0.51.0% of the world population.
The American Rheumatism Association criteria for the classification of RA :
* morning stiffness, * arthritis of three or more joint areas, * arthritis of hand joints, * symmetric arthritis, * rheumatoid nodules, * serum rheumatoid factor (RF) * radiographic changes A patient should have four of the seven criteria to be diagnosed
with RA and the first four criteria should be present for at least six weeks.
-
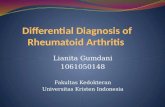
Autoimmune processes are predicted to occur up to years prior to the clinical onset of disease and represent a pre-articular or lymphoid phase of disease. Transition to the articular phase, which corresponds to the clinical manifestation of the disease, is initiated by ill-defined processes, such as biomechanical
and neurological events. Thereafter inflammation-driven pathogenesis occurs, which leads to joint destruction and increases co-morbidity, including cardiovascular disease and osteoporosis. Autoimmune processes may defer to inflammatory pathways as the disease progresses. CCP, cyclic citrullinated peptide; CTLA4, cytotoxic T-lymphocyte antigen 4; GP39, cartilage glycoprotein 39; PADI4, peptidyl arginine deiminase, type IV; PTPN22, protein tyrosine
phosphatase, non-receptor type 22.
-
SISTEM GEN HLASISTEM GEN HLA
-
Environmental factors * Exposure to bacteria Mycoplasma
organisms, Epstein-Barr virus, rubella virus, and Streptococcus,
* A particular diet a lack of Vitamin C * Smoking a major environmental risk
factor
-
Systemic Acute Inflammatory ResponseSystemic Acute Inflammatory Response
Prostaglandins FeverHypothalamus
Local acute inflammatory response
Adrenal cortex
ACTH (via pituitary)
IL-1, TNF , IL-6, LIF, OSM
Liver
Acute phase proteins :
C-reactive protein (CRP)
Serum amyloid A (SAA)
Fibrinogen
Mannose-binding protein
Complement component
IL-6, TNF Leukocytosis
Bone marrow
CorticosteroidsIL-
1,TN
F , IL
-6
-
Gambaran utama :Gambaran utama :
Auto imunitas Inflamasi kronis Kerusakan sendi
-
Patogenesis RAPatogenesis RA
Terkait MHC kelas II TH-1 cell mediated
-
Figure 5-2Figure 5-2
-
Synovial T cells may be activated by T-cell receptor (TCR) and co-stimulation pathways and by cytokine- or Toll-like receptor (TLR)-driven stimuli. In particular, the synovial milieu contains interleukin-12 (IL-12), IL-23, IL-6 and transforming growth factor- (TGF ), and as such promotes the differentiation of T helper 1
(TH1) and TH17 cells. Regulatory T cells, although present, may not exhibit optimal regulatory activity. In rodent models, regulatory T cells are present in high numbers in the joints, whereas in human disease the relative contribution of these subsets remains unknown. Activated T cells mediate effector function in
rheumatoid arthritis through the release of cytokines, to promote downstream leukocyte and mesenchymal-cell activation, through the provision of help to B cells and, in the case of CD8+ effector T cells, cytotoxic activity. They also activate macrophages, fibroblasts and endothelial cells through direct cell contact. CD40L, CD40 ligand; GM-CSF, granulocyte/macrophage colony-stimulating factor; RANKL, receptor activator of nuclear factor- B (RANK) ligand; IFN , interferon- ; TNF,
tumour-necrosis factor.
-
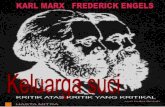
The component cells of the inflamed rheumatoid synovial membrane are depicted in innate and adaptive predominant compartments of the inflammatory response. Pivotal cytokine pathways are depicted in which activation of dendritic cells (DCs), T cells, B cells and macrophages underpins the dysregulated expression of cytokines that in turn drive activation of effector cells, including neutrophils, mast cells, endothelial cells and synovial fibroblasts. The clinical manifestations of such effects are highlighted. Only key cytokines are shown in each domain for relative simplicity; the main text contains more detailed
description of the precise role of additional cytokines in these processes. Bidirectional arrows represent a relationship between cells that is influenced by the cytokines listed. The pathways that lead to tissue destruction via osteoclast and chondrocyte activation are detailed in Figs 4,5. APRIL, a proliferation-inducing ligand; BAFF, B-cell activating factor; bFGF, basic fibroblast growth factor; CCL21, CC-chemokine ligand 21; CXCL13, CXC-chemokine ligand 13; FcgR, Fc
receptor for IgG; IFN, interferon; IL, interleukin; LT , lymphotoxin- ; M-CSF, macrophage colony-stimulating factor; PAR2, protease-activated receptor 2; RANKL, receptor activator of nuclear factor- B (RANK) ligand; TGF , transforming growth factor- ; TH, T helper; TLR, Toll-like receptor; TNF, tumour-necrosis factor;
VEGF, vascular endothelial growth factor.
-
Kerusakan sendi pada RAKerusakan sendi pada RA
Osteoklas pada sisi antara jaringan sinovial dan tulang sendi menginduksi resorbsi tulang invasi sel membran sinovial pannus
-
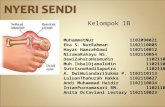
AKTIVITAS RESORBSI TULANG PADA RA
The essential cytokine mediators are RANKL (receptor activator of nuclear factor- B (RANK) ligand) and M-CSF (macrophage colony-stimulating factor), which are expressed by synovial fibroblasts and T helper 1 (TH1) cells. Osteoclast differentiation is achieved by the actions of tumour-necrosis factor (TNF) and
interleukin-1 (IL-1), as well as of IL-17, produced by TH17 cells, and IL-7, produced by synovial fibroblasts. By contrast, IL-4 and IL-10, which are produced by TH2 cells, and granulocyte/M-CSF (GM-CSF) and interferon- (IFN ), which are produced by TH1 cells, inhibit osteoclast differentiation.
-
Cartilage degradation is a multistep process based on the release of matrix-degrading enzymes such as aggrecanases (ADAMTS) and matrix metalloproteinases (MMPs). Cytokines such as interleukin-1 (IL-1) and IL-17 induce a switch in the synthesis pattern of chondrocytes from matrix molecules to matrix-degrading enzymes. In addition, synovial fibroblasts start producing matrix-degrading enzymes and invade cartilage when activated by cytokines such as
tumour-necrosis factor (TNF) and IL-1. Chondrocyte death is another feature of cartilage damage, it leads to the formation of empty lacunae and deprives cartilage from the ability to replenish matrix.
MEKANISME DISINTEGRASI TULANG RAWAN PADA RA
-
BIOMARKERBIOMARKER
Defined as a structural or physical measure, or a cellular, molecular, or genetic change or feature by which alterations in a biologic process can be identified and monitored.
may thereby have diagnostic or prognostic utility
measuring the intended analyte and/or process with sufficient specificity
-
BIOMARKER in RABIOMARKER in RA
Biomarker of autoantibody Biomarker of bone turnover Biomarker of cartilage turnover
-
BIOMARKER of AUTOANTIBODIBIOMARKER of AUTOANTIBODI
Rheumatoid Factor (RF) Anti-CCP Antibodies * includes a group of autoantibodies with
shared reactivity for proteins containing arginine residues that have been modified to citrulline
* includes : antiperinuclear factor (APF), antikeratin antibody (AKA), and antifilaggrin antibody (AFA)
-
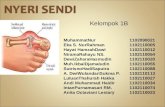
Possible links between rheumatoid arthritis (RA) specific anti-cyclic citrullinated peptide (anti-CCP) antibodies and RA-associated genetic factors.
(a) PADI4 single nucleotide polymorphisms (SNPs) may lead to elevated PAD4 expression and to increased citrullination of proteins (b) RA-associated HLA-DR4 molecules (DR4) can bind and present citrullinated peptides much more efficiently than noncitrullinated peptides (c) IL-10 promoter SNPs are associated with increased anti-CCP antibody production and severity of the disease (d) Various cytokine polymorphisms are associated with RA and may lead to stronger effects of immune complex activated cells.
-
KONVERSI ENZIMATIK ARGININ SITRULIN
-
Anti-CCP AntibodiesAnti-CCP Antibodies Has a remarkably high specificity for
RA, of the order 98%, which is superior to that of RF
Predictive of progression to erosive RA and a more severe disease course
Determined early in the course of RA are good predictors of radiographic joint damage
Combined with RF provides the most accurate prediction of erosive disease
-
European League Against Rheumatism European League Against Rheumatism (EULAR) (EULAR) RecommendationsRecommendations : :
In every patient presenting with early arthritis to the rheumatologist, the following factors predicting persistent and erosive disease should be measured by:
Number of tender and swollen joints ESR or CRP Levels of rheumatoid factor and anti-CCP
antibodies Radiographic erosions
-
BIOMARKER of BONE TURNOVERBIOMARKER of BONE TURNOVER
Markers of bone formation Serum osteocalcin, serum bone-specific alkaline
phosphatase, and serum levels of N- and C-propeptides of type I procollagen (PINP and PICP)
Markers of bone resorption (degradation) Urinary pyridinoline (PYD) and deoxypyridinoline
(DPD), urinary and serum levels of the N- and C-telopeptides of type I collagen (NTX and CTX), and serum levels of tartrate-resistant acid phosphatase 5b (TRACP-5b)
-
BIOMARKER of CARTILAGE TURNOVERBIOMARKER of CARTILAGE TURNOVER
Markers of Cartilage Degradation Urine CartiLaps (CTX-II), cartilage oligomeric
matrix protein (COMP), human cartilage glycoprotein 39 (HC gp-39; YKL-40)
Markers of Cartilage Synthesis N- and C-propeptides of type II procollagen
and the chondroitin sulphate (CS) 846 epitope of aggrecan
-
PRA ANALITIKPRA ANALITIK
Variasi biologis Asupan makanan Status renal dan hepatik pasien
-
VARIASI BIOLOGISVARIASI BIOLOGIS
Terutama berpengaruh pada pengukuran petanda degradasi tulang
Variasi hingga 50 70 % dari kadar rerata
Perhatikan waktu pengambilan spesimen !
-
PENGARUH ASUPAN MAKANANPENGARUH ASUPAN MAKANAN
Terutama pada petanda resorbsi tulang (CTX-1, NTX)
Pengambilan spesimen pada pasien puasa
Pengaruh pada petanda cartilage turnover (?) Exercise COMP
-
STATUS RENAL & HEPATIK PASIENSTATUS RENAL & HEPATIK PASIEN
Tergantung organ ekskretor biomarker
CTX-1, NTX, PINP, Osteoklasin diekskresi oleh ginjal
TRACP, BSAP diekskresi hepar
-
BIODATARHEUMATOID ARTHRITIS FROM BASIC TO CLINICSlide 3Slide 4Slide 5Slide 6Slide 7Slide 8Systemic Acute Inflammatory ResponseGambaran utama :Slide 11Patogenesis RAFigure 5-2Slide 14Slide 15Slide 16Slide 17Slide 18Slide 19Kerusakan sendi pada RASlide 21Slide 22Slide 23Slide 24BIOMARKERBIOMARKER in RABIOMARKER of AUTOANTIBODISlide 28Slide 29Anti-CCP AntibodiesEuropean League Against Rheumatism (EULAR) Recommendations :BIOMARKER of BONE TURNOVERBIOMARKER of CARTILAGE TURNOVERPRA ANALITIKVARIASI BIOLOGISPENGARUH ASUPAN MAKANANSTATUS RENAL & HEPATIK PASIENSlide 38Slide 39