Ma Rasmus

of 13
description
marasmus
Transcript of Ma Rasmus
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 1/13
Marasmus
Author: Simon S Rabinowitz, MD, PhD, FAAP; Chief Editor: Jatinder Bhatia, MBBS more...
Updated: Mar 22, 2012
Background
Marasmus is one of the 3 forms of serious protein-energy malnutrition (PEM). The other 2 forms are kwashiorkor(KW) and marasmic KW. These forms of serious PEM represent a group of pathologic conditions associated witha nutritional and energy deficit occurring mainly in young children from developing countries at the time of weaning.Marasmus is a condition primarily caused by a deficiency in calories and energy, whereas kwashiorkor indicatesan associated protein deficiency, resulting in an edematous appearance. Marasmic kwashiorkor indicates that, inpractice, separating these entities conclusively is difficult; this term indicates a condition that has features of both.[1, 2]
These conditions are frequently associated with infections, mainly GI. The reasons for a progression of nutritionaldeficit into marasmus rather than kwashiorkor are unclear and cannot be solely explained by the composition ofthe deficient diet (ie, a diet deficient in energy for marasmus and a diet deficient in protein for kwashiorkor). Thestudy of these phenomena is considerably limited by the lack of an appropriate animal model. Unfortunately, manyauthors combine these entities into one, thus precluding a better understanding of the differences between theseclinical conditions.
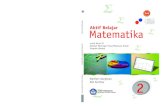
Marasmus is a serious worldwide problem that involves more than 50 million children younger than 5 years.According to the World Health Organization (WHO), 49% of the 10.4 million deaths occurring in children youngerthan 5 years in developing countries are associated with PEM.
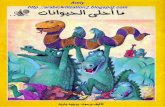
See the image below.
Malnutrition hotspot map. Image courtesy of the World Health Organization (WHO) and United Nations Children's Fund (UNICEF).
Malnutrition has been a permanent priority of the WHO for decades. Although a higher proportion of severelymalnourished children do not survive a significant intercurrent illness, as much as 80% of the overall, unacceptablyhigh, mortality rate may be contributed by mild-to-moderately malnourished children because this cohort is so
much higher.[3] Accordingly, newer strategies need not be limited to only severely malnourished children.
Although PEM occurs more frequently in low-income countries, numerous children from higher-income countries
Today NewsReferenceEducationLog Out My AccountDr. A Hariyanto
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 2/13
are also affected, including children from large urban areas and of low socioeconomic status, children with chronicdisease, and children who are institutionalized. Recently, studies of hospitalized children from developed countrieshave demonstrated an increased risk for PEM. Risk factors include a primary diagnosis of mental retardation,cystic fibrosis, malignancy, cardiovascular disease, end stage renal disease, oncologic disease, genetic disease,
neurological disease, multiple diagnoses, PICU admission, or prolonged hospitalization.[4, 5] In these conditions,the challenging nutritional management is often overlooked and underestimated, resulting in an impairment of thechances for recovery and the worsening of an already precarious neurodevelopmental situation.
PEM results in not only high mortality (even for hospitalized children), without any improvement over the last 2decades, and also results in morbidity, stunted linear growth, and compromised neurological development. Thesocial and economic implications of PEM and its complications are incalculable.
This article focuses mainly on marasmus that results from an insufficient nutritional intake as observed underimpaired socioeconomic conditions, such as those present in developing countries. Marasmus is most frequentlyassociated with acute infections (eg, gastroenteritis, respiratory illnesses, measles), chronic illnesses (eg,tuberculosis, HIV infection) or drastic natural or man made conditions (eg, floods, droughts, civil war).
Pathophysiology
Various extensive reviews of the pathophysiological processes resulting in marasmus are available. Unlikekwashiorkor, the clinical sequelae of marasmus can be considered as an evolving adaptation in a child facing aninsufficient energy intake. Marasmus always results from a negative energy balance. The imbalance can resultfrom a decreased energy intake, an increased loss of ingested calories (eg, emesis, diarrhea, burns), an increasedenergy expenditure, or combinations of these factors, such as is observed in acute or chronic diseases. Childrenadapt to an energy deficiency with a decrease in physical activity, lethargy, a decrease in basal energymetabolism, slowing of growth, and, finally, weight loss.
Pathophysiological changes associated with nutritional and energy deficits can be described as (1) bodycomposition changes, (2) metabolic changes, and (3) anatomic changes.
Body Composition
Body mass: Body mass is significantly decreased in a heterogeneous way.Fat mass: Fat stores can decrease to as low as 5% of the total body weight and can be macroscopicallyundetectable. The remaining fat is usually stored in the liver, giving a paradoxical appearance of a fatty liver.Although this is often observed in kwashiorkor, it also occurs to a lesser extent in marasmus. A study from
Nigeria examined serum lipids in malnourished children.[6] These authors found that total cholesterol, lowdensity lipoprotein cholesterol, and high density lipoprotein cholesterol levels were significantly higher inchildren with kwashiorkor than in those with marasmus.Total body water: The proportion of water content in the body increases with the increased seriousness ofPEM (marasmus or kwashiorkor) and is associated with the loss of fat mass, which is poor in water. Theproportion of extracellular water also increases, often resulting in edema. Edema is significant inkwashiorkor but can also be present in marasmus or in the frequently encountered mixed forms of PEM.The increase in extracellular water is proportional to the increase in the total body water. During the firstdays of therapy, part of the extracellular water shifts to the intracellular compartment and part of it is lost inthe urine, resulting in the observed initial weight loss with treatment.Protein mass: Mainly represented by muscle and some organs (eg, heart), protein mass can decrease asmuch as 30% in the most serious forms. The muscle fibers are thin with loss of striation. Muscle cells areatrophic, and muscle tissue is infiltrated with fat and fibrous tissue. Total recovery is long but appears to bepossible.Other organ mass: The brain, skeleton, and kidney are preserved, whereas the liver, heart, pancreas, anddigestive tract are first affected.Pediatric and adult physiologic change: Finally, physiologic changes are different in infants and childrenwhen compared with adults. For example, infants with marasmus have an increased tendency tohypothermia and hypoglycemia, requiring the frequent administration of small meals. This can be explainedby the body composition imbalance of children with marasmus in favor of high-energyconsuming organs,
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 3/13
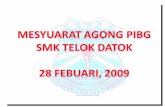
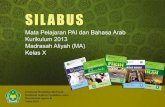
such as the brain and kidney, compared with energy-storage organs, such as muscle and fat.Assessment of fat and muscle mass: As described below, assessment of the fat and muscle mass losscan be clinically performed by measuring arm circumference (see image below) or skinfold thickness, suchas triceps skinfold. The diagram illustrates the validity of this assessment method. Because armcircumference is relatively constant in healthy children aged 1-5 years, it roughly represents a generalassessment of nutritional status.
Physiopathological principle of arm circumference measurement in children aged 1-5 years and the relationship w ith severity of
malnutrition.
Minerals and Vitamins
Potassium: Potassium is the electrolyte most studied in marasmus. Total body potassium deficit isassociated with decreased muscle mass, poor intake, and digestive losses. This potassium deficit, whichcan reach 15 mEq/kg, contributes to hypotonia, apathy, and impaired cardiac function.Other electrolytes: Plasma sodium concentration is generally within the reference range, but it can be low,which is then a sign of a poor prognosis. However, intracellular sodium level is elevated in the brain,muscle, and red and white blood cells, explaining the sodium excretion in the first days of recovery.Other minerals: A deficit in calcium, phosphorus, and magnesium stores is also observed. Iron deficiencyanemia is consistently observed in marasmus. However, in the most serious forms, iron accumulates in theliver, most likely because of the deficit in transport protein. These patients are at higher risk of mortality;therefore, iron is supplemented only after the acute recovery phase is completed. Zinc, selenium, andmagnesium are more significantly reduced in kwashiorkor but are also constantly deficient in marasmus.Several studies have shown improved recovery from malnutrition and decreased mortality withsupplementation of these 3 micronutrients. A Cochrane review concluded that zinc supplementation isclearly of benefit in children aged 6 months or older with diarrheal diseases in areas where these conditions
are an important cause of childhood mortality.[7]
Vitamins: Both fat-soluble vitamins (ie, A, D, E, K) and water-soluble vitamins (eg, B-6, B-12, folic acid)must be systematically administered. Vitamin A is essential to retinal function, has a trophic effect onepithelial tissues, and plays a major role as an antioxidant agent. Vitamin A deficit affects visual function(eg, conjunctivitis, corneal ulcer, night blindness, total blindness) and digestive, respiratory, and urinaryfunctions. Furthermore, vitamin A supplementation programs have resulted in decreased mortality andmorbidity, in particular, during diarrheal disease and measles.
Vitamin and micronutrient deficiencies can be differentiated in 2 categories listed below. Patients with deficienciesof type 1 nutrients present with late and specific clinical signs. In contrast, patients with deficiencies of type 2nutrients are difficult to identify because blood levels are unreliable and the clinical signs are nonspecific, such asthe growth retardation with mild deficiency and weight loss with significant deficiency. Furthermore, type 2 nutrientdeficiencies are often combined. Therefore, these deficiencies are global and require a global nutritionalrehabilitation, such as WHO standardized solution.
Below are characteristics of type 1 and type 2 deficiencies, according to Golden from a 1991 report.
Type 1 deficienciesSpecific clinical signsClinical signs appear after a latency period
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 4/13
Used in specific metabolic pathwaysAre independent of one anotherVariable tissue concentration
Type 2 deficienciesNonspecific clinical signsNutrient status related to daily intakeUsed in various organs and metabolic pathwaysNutrient interactionConstant tissue concentration
Below are lists of nutrient classification according to the clinical response to deficiency in type 1, with reduction oftissue concentration, and type 2 with growth deficit.
Type 1 nutrientsSeleniumIodineIronCopperCalciumManganeseThiaminRiboflavinAscorbic acidRetinolTocopherolCalciferolFolic acidB-12 vitaminPyridoxine
Type 2 nutrientsSodiumSulfurEssential amino acidsPotassiumSodiumMagnesiumZincPhosphorusWater
Metabolic Changes
The overall metabolic adaptations that occur during marasmus are similar to those in starvation, which have beenmore extensively investigated. The primary goal is to preserve adequate energy to the brain and other vital organsin the face of a compromised supply. Early on, a rise in gluconeogenesis leads to a perceived increased metabolicrate. As fasting progresses, gluconeogenesis is suppressed to minimize muscle protein breakdown, and ketonesderived from fat become the main fuel for the brain.
With chronic underfeeding, the basal metabolic rate decreases. One of the main adaptations to long-standingenergy deficiency is a decreased rate of linear growth, yielding permanent stunting. The energy saving is partiallyattenuated by the diversion of energy from muscle to the more metabolically active organs. Further adaptations tocrisis situations, such as significant infections, may have some parallels to those that are observed in a stressed,
malnourished animal model.[8] The rise in energy expenditure and urinary nitrogen excretion following surgery weresignificantly less in malnourished rats. This suggests that malnutrition can impair the ability of the organism tomobilize substrates to respond to stress. However, the healing process in these animals remained normal,indicating the ability to prioritize this biological activity.
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 5/13
Energy metabolismWith reduced energy intake, a decrease in physical activity occurs followed by a progressivelyslower rate of growth. Weight loss initially occurs due to a decrease in fat mass, and afterwards by adecrease in muscle mass, as clinically measured by changes in arm circumference (see imagebelow).
Physiopathological principle of arm circumference measurement in children aged 1-5 years and the relationship w ith
severity of malnutrition.
Muscle mass loss results in a decrease of energy expenditure. Reduced energy metabolism canimpair the response of patients with marasmus to changes in environmental temperature, resulting inan increased risk of hypothermia. Furthermore, during infection, fever is reduced compared to a well-nourished patient. In case of nutrient deficiency, the metabolism is redirected to vital function(requiring 80-100 kcal/kg/d). During recovery, the energy cost of catch-up growth has to be added(up to 100 kcal/kg/d). At this stage, energy needs can be massive.
Protein metabolism: Intestinal absorption of amino acids is maintained, despite the atrophy of the intestinalmucosa. Protein turnover is decreased (as much as 40% in severe forms), and protein-sparing mechanismsregulated by complex hormonal controls redirect amino acids to vital organs. Amino acids liberated fromcatabolism of muscle are recycled by the liver for the synthesis of essential proteins. Total plasma proteins,including albumin, are decreased, whereas gamma globulins are often increased by the associatedinfections.Albumin: An albumin concentration lower than 30 g/L is often considered as the threshold below whichedema develops from decreased oncotic pressure. However, in marasmus, albumin concentration canoccasionally be below this value without edema. Prealbumin concentration is a sensitive index of proteinsynthesis. It decreases with decreased protein intake and rapidly increases in a few days with appropriatenutritional rehabilitation. Insulinlike growth factor 1 (IGF-1) is another sensitive marker of nutritional status.Carbohydrate metabolism: This has mainly been studied in order to explain the serious and often fatalhypoglycemia that occurs in the initial renutrition phase of children with marasmus. The glucose level isoften initially low, and the glycogen stores are depleted. Also, a certain degree of glucose intolerance ofunclear etiology is observed, possibly associated with a peripheral resistance to insulin or withhypokalemia. In the initiation of renutrition or in association with diarrhea or infection, a significant risk ofprofound and even fatal hypoglycemia occurs. Small and frequent meals are recommended, including duringthe night, to avoid death in the early morning. Furthermore, the digestion of starch is impaired by thedecreased production of pancreatic amylase. Lactose malabsorption is frequent but is generally withoutclinical consequences. In most cases, renutrition using milk is possible.Fat metabolism: Dietary fats are often malabsorbed in the initial phase of marasmus renutrition. Themobilization of fat stores for energy metabolism takes place under hormonal control by adrenaline andgrowth hormone. Blood lipid levels are usually low, and serious dysregulation of lipid metabolism can occur,mainly during kwashiorkor and rarely during marasmus.
Anatomic Changes
Digestive tract
The entire digestive tract from mouth to rectum is affected. The mucosal surface becomes smooth and thin, and
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 6/13
secretory functions are impaired. A decrease in gastric hydrochloric acid (HCl) excretion and a slowing ofperistalsis is observed, yielding bacterial overgrowth in the duodenum. Proportionally, the digestive tract is theorgan system that loses the largest mass during marasmus. However, these important alterations of the digestivetract interfere only moderately with normal nutrient absorption. Therefore, early enteral renutrition is notcontraindicated but is encouraged because some of the nutrients necessary for the recovery of the intestinalmucosa are used directly from the lumen.
In addition to the anatomic changes associated with PEM, the frequent intestinal infections by viruses andbacteria and the toxins they produce also contribute to the changes in the digestive tract. Liver volume usuallydecreases, as do other organ volumes. An enlarged liver suggests the possibility of other diagnoses, such askwashiorkor or hepatitis. Liver synthetic function is usually preserved, although protein synthesis is decreased, asreflected by the decreased albumin and prealbumin levels. Glycogen synthesis is decreased, further increasing therisk for hypoglycemia. The detoxifying function of the liver is impaired with structural changes in the liver cells.Therefore, drugs that are metabolized by the liver should be administered with caution, and liver function should bemonitored.
Endocrine system
Many of the adaptations seen in marasmus are mediated by thyroid hormones, insulin, and growth hormone. As inany stressed state, the adrenergic response is activated (see image below).
Hormonal adaptation to the stress of malnutrition. The evolution of marasmus.
This response is functional in marasmus but less so in kwashiorkor. Muscle proteins are converted into aminoacids and are used for the hepatic synthesis of lipoproteins. These lipoproteins contribute to the mobilization oftriglycerides from the liver. In contrast, during kwashiorkor, this function is impaired, resulting in liver steatosis,which is not usually present in marasmus. However, any precipitating factor, such as gastroenteritis orinappropriate renutrition, can disrupt this fragile adaptive mechanism.
Furthermore, in serious marasmus, a significant degree of hypothyroidism, with a decrease in the size of thethyroid gland and repercussions on the brain function and psychomotor development exists. In less severe forms,the impaired thyroid function has fewer clinical consequences. Insulin levels are low and contribute to a certaindegree of glucose intolerance, especially during kwashiorkor. Therefore, high-carbohydrate diets are inappropriate.Growth hormone levels are initially within the reference range, but they progressively decrease with time,explaining the halt in linear growth observed with marasmus.
After initiation of renutrition, the hormonal milieu is reversed allowing for substantial anabolism and a rapid lineargrowth spurt. However, if the marasmic state has gone on too long, then the adult height is less than the geneticpotential. Recently, investigators have obtained data that suggest a role for additional hormones in PEM. Levels of
serum gherlin(an appetite stimulating peptide) were increased[9] and serum levels of leptin (a satiety hormone) and
IGF-1 were decreased in children with PEM compared with healthy controls.[10]
Hematopoietic system
A moderate normochromic or slightly hypochromic anemia is usually present, with normal RBC size. Iron andfolate deficiencies, intestinal parasites, malaria, and other chronic infections exacerbate the anemia. However, ironstores are present in the liver. Therefore, iron supplementation should not be initially implemented. Oral iron ispoorly tolerated by the digestive tract. The other blood cells (eg, thrombocytes, WBCs) are also affected, but with
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 7/13
generally limited clinical consequences. Blood clotting mechanisms are usually preserved, except in the case ofserious vitamin K deficiency.
Immune system
Immune impairment and infections are usually associated with marasmus. Thymus atrophy is a characteristicmanifestation of marasmus, but all T lymphocyteproducing tissues are affected. However, B-lymphocyte tissues,such as Peyer patches, the spleen, and the tonsils, are relatively preserved. Cellular immunity is most affected,with a characteristic tuberculin anergy. However, antibody production is maintained. In marasmus, a generalacquired immunodeficiency occurs, with a decrease in secretory immunoglobulin A (IgA) and an impairment of thenonspecific local defense system, such as mucosal integrity and lymphokine production. Bacteriemia,candidiasis, and Pneumocystis carinii infection are frequently present. Immune impairment is less frequent withmoderate malnutrition. Immunological recovery is generally rapid, except if measles is associated.
Brain and nervous system
Cerebral tissue is usually preserved during marasmus. Brain atrophy with impairment of cerebral functions is onlypresent in severe forms of marasmus. Effects on the brain are more important if malnutrition takes place during thefirst year of life or during fetal life. Irritability and apathy are characteristic of marasmus but improve rapidly withrecovery. The permanent developmental consequences of marasmus are difficult to evaluate. Ongoing studies areevaluating these long-term consequences, as well as the benefit of nutritional supplementation with variousvitamins and minerals.
Cardiovascular system
Cardiac muscle fiber is thin, and the contractility of the myofibrils is impaired. Cardiac output, especially systolicfunction, is decreased in the same proportion as the weight loss. Bradycardia and hypotension commonly occur insevere forms of malnutrition. Electrolyte imbalances present during marasmus modify the ECG findings. With thisimpaired cardiac function, any increase of intravascular volume during rehydration or blood transfusion can result ina significant cardiac insufficiency. With the rapid metabolic, energy, and electrolyte changes of the initial phase ofrenutrition, this period is also a period of high risk for arrhythmia or cardiac arrest. Therefore, close clinicalmonitoring is critical in children with circulatory compromise.
Epidemiology
Frequency
United States
Marasmus is rarely reported in American children. In 1995, 228 deaths were attributed to marasmus in the UnitedStates. Most of these deaths were in elderly adults, and only 3 occurred in children. However, these data do notinclude deaths associated with marasmus complicating anorexia nervosa.
Incidence of nonfatal marasmus is unclear in the United States because most patients have an underlyingcondition, and marasmus is not reported as an admission or discharge diagnosis. However, a report from a tertiarycare center in Massachusetts reported prevalence rates of severe (1.3%), moderate (5.8%), and mild (17.4%)
acute PEM in hospitalized children, based on the Waterlow criteria.[11] In the same cohort, chronic PEM (deficitsin height for age) was found to be severe (5.1%), moderate (7.7%), and mild (14.5%).
Acute (33%) and chronic (64%) malnutrition, based on comparing weight and height with controls, was foundamong a cohort of 160 children hospitalized with congenital heart disease in a regional pediatric cardiothoracic
center at the University of Michigan.[12] Malnutrition was inversely correlated with age and was present in 80% ofthe hospitalized infants. These studies, as well as reports from Western Europe, suggest that marasmus is
underappreciated amongst chronically ill children in the United States.[3, 4]
International
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 8/13
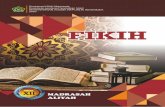
Nearly 30% of humans currently experience one or more of the multiple forms of malnutrition. Close to 50 millionchildren younger than 5 years have PEM, and half of the children who die younger than 5 years are undernourished(see image below). Approximately 80% of these malnourished children live in Asia, 15% in Africa, and 5% in Latin
America.[13]
Distribution of 10.4 million deaths among children younger than 5 years in all developing countries. World health Organization (WHO),
1995.
Because as many as 20-30% of severely malnourished children die during treatment by the health services,[14]
interest in reporting the prevalence of malnutrition in hospitalized children in different countries has been renewed.A recent review article estimated the prevalence of acute malnutrition over the last 10 years in hospitalized childrenin Germany, France, the United Kingdom, and the United States to be 6.1-14%; the prevalence is as much as
32% in Turkey.[4] However, a recent German study determined that the prevalence of malnutrition was even higher(24% with 1.7% severe, 4.4% moderate, and 17.7% mild) in a cohort of unselected children admitted to a large
tertiary care children's hospital in 2003-2004.[5] Furthermore, a worsening of nutritional status in hospitalized
children in Brazil,[15] France,[16] and Turkey.[17]
Paradoxically, a massive global epidemic of obesity, especially in countries in rapid economic transition, issimultaneously emerging in children and adolescents.
Mortality/Morbidity
Five million children younger than 5 years die every year of malnutrition. Approximately 70 million present withwasting, and 230 million present with some stunting. Fifty percent of the children in Asia are malnourished, 30%are malnourished in Africa, and 20% are malnourished in Latin America.
Race
No racial predilection in the prevalence of malnutrition is evident, but a strong association with the geographicdistribution of poverty is observed.
Sex
No sexual predilection is observed, although, in some parts of the world, cultural practices place girls at adisadvantage for PEM.
Age
Marasmus is more frequent in children younger than 5 years because this period is characterized by increasedenergy needs and increased susceptibility to viral and bacterial infections. Weaning, which occurs during thisperiod, is often complicated by factors such as geography (eg, drought, poor soil productivity), economy (eg,illiteracy, unemployment), hygiene (eg, access to quality water), public health (eg, number of nurses is more thannumber of physicians), and culture and dietetics (eg, intrafamily distribution of high-nutrition foods).
Contributor Information and DisclosuresAuthorSimon S Rabinowitz, MD, PhD, FAAP Professor of Clinical Pediatrics, Vice Chairman, Clinical PracticeDevelopment, Pediatric Gastroenterology, Hepatology, and Nutrition, State University of New York DownstateCollege of Medicine, The Children's Hospital at Downstate
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 9/13
Simon S Rabinowitz, MD, PhD, FAAP is a member of the following medical societies: American Academy ofPediatrics, American Association for the Advancement of Science, American College of Gastroenterology,American Gastroenterological Association, American Medical Association, New York Academy of Sciences,North American Society for Pediatric Gastroenterology and Nutrition, Phi Beta Kappa, and Sigma Xi
Disclosure: Abbott nutrition Honoraria Speaking and teaching
Coauthor(s)Mario Gehri, MD Consulting Staff, Department of Pediatrics, Hpital De L'Enfance, Centre HospitalierUniversitaire Vaudois, Switzerland
Disclosure: Nothing to disclose.
Ermindo R Di Paolo, PhD Pharmacist, Department of Pharmacy, University Hospital CHUV, Lausanne,Switzerland
Disclosure: Nothing to disclose.
Natalia M Wetterer, MD Resident Physician, Department of Pediatrics, New York Medical College
Disclosure: Nothing to disclose.
Esther N Prince, MD Pediatric Gastroenterology Fellow, State University of New York Downstate MedicalCenter
Disclosure: Nothing to disclose.
Specialty Editor BoardMaria Rebello Mascarenhas, MBBS Associate Professor of Pediatrics, University of Pennsylvania School ofMedicine; Section Chief of Nutrition, Division of Gastroenterology and Nutrition, Director, Nutrition SupportService, Children's Hospital of Philadelphia
Maria Rebello Mascarenhas, MBBS is a member of the following medical societies: AmericanGastroenterological Association, American Society for Parenteral and Enteral Nutrition, and North AmericanSociety for Pediatric Gastroenterology and Nutrition
Disclosure: The 5-minute pediatric consult Royalty editor
Mary L Windle, PharmD Adjunct Associate Professor, University of Nebraska Medical Center College ofPharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Nothing to disclose.
Jatinder Bhatia, MBBS Professor of Pediatrics, Chief, Section of Neonatology, Department of Pediatrics,Medical College of Georgia
Jatinder Bhatia, MBBS is a member of the following medical societies: American Academy of Pediatrics,American Association for the Advancement of Science, American Dietetic Association, American PediatricSociety, American Society for Clinical Nutrition, American Society for Parenteral and Enteral Nutrition, Societyfor Pediatric Research, and Southern Society for Pediatric Research
Disclosure: Nothing to disclose.
Merrily P M Poth, MD Professor, Department of Pediatrics and Neuroscience, Uniformed Services Universityof the Health Sciences
Merrily P M Poth, MD is a member of the following medical societies: American Academy of Pediatrics,Endocrine Society, and Pediatric Endocrine Society
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 10/13
Disclosure: Nothing to disclose.
Chief EditorJatinder Bhatia, MBBS Professor of Pediatrics, Chief, Section of Neonatology, Department of Pediatrics,Medical College of Georgia
Jatinder Bhatia, MBBS is a member of the following medical societies: American Academy of Pediatrics,American Association for the Advancement of Science, American Dietetic Association, American PediatricSociety, American Society for Clinical Nutrition, American Society for Parenteral and Enteral Nutrition, Societyfor Pediatric Research, and Southern Society for Pediatric Research
Disclosure: Nothing to disclose.
Additional ContributorsThe authors and editors of Medscape Reference gratefully acknowledge the use of images and information fromthe United Nations Children's Fund (UNICEF).
References
1. Scrimshaw NS, Viteri FE. INCAP studies of kwashiorkor and marasmus. Food Nutr Bull. Mar2010;31(1):34-41. [Medline].
2. Spoelstra MN, Mari A, Mendel M, Senga E, van Rheenen P, van Dijk TH, et al. Kwashiorkor andmarasmus are both associated with impaired glucose clearance related to pancreatic -cell dysfunction.Metabolism. Mar 2 2012;[Medline].
3. Pelletier DL, Frongillo EA Jr, Schroeder DG, Habicht JP. The effects of malnutrition on child mortality indeveloping countries. Bull World Health Org. 1995;73 (4):443-8. [Medline].
4. Joosten KF, Hulst JM. Prevalence of malnutrition in pediatric hospital patients. Curr Opin Pediatr. Oct2008;20(5):590-6. [Medline].
5. Pawellek I, Dokoupil K, Koletzko B. Prevalence of malnutrition in paediatric hospital patients. Clin Nutr.Feb 2008;27(1):72-6. [Medline].
6. Akuyam SA, Isah HS, Ogala WN. Serum lipid profile in malnourished nigerian children in zaria. NigerPostgrad Med J. September 2008;15 (3):192-6.
7. Emery PW. Metabolic changes in malnutrition. Eye. October 2005;19 (10):1029-32. [Medline].
8. [Best Evidence] Lazzerini M, Ronfani L. Oral zinc for treating diarrhoea in children. Cochrane DatabaseSyst Rev. 2008;(3):CD005436. [Medline].
9. Altinkaynak S, Selimoglu MA, Ertekin V, Kilicarslan B. Serum ghrelin levels in children with primaryprotein-energy malnutrition. Pediatr Int. Aug 2008;50(4):429-31. [Medline].
10. Kilic M, Taskin E, Ustundag B, Aygun AD. The evaluation of serum leptin level and other hormonalparameters in children with severe malnutrition. Clin Biochem. May 2004;37(5):382-7. [Medline].
11. Hendricks KM, Duggan C, Gallagher L, et al. Malnutrition in hospitalized pediatric patients. Currentprevalence. Arch Pediatr Adolesc Med. Oct 1995;149(10):1118-22. [Medline].
12. Cameron JW, Rosenthal A, Olson AD. Malnutrition in hospitalized children with congenital heart disease.Arch Pediatr Adolesc Med. Oct 1995;149(10):1098-102. [Medline].
13. Fisberg M, Nobrega FJ. Disturbios da nutricao. Revinter. 1998;140-4.
14. Manejo da desnutricao grave: um manual para profissionals de saude de nivel superior (medicos,enfermeiros, nutricionistas e outros) e suaas equipes auxillares. Organizacao Mundial da Saude, Brasilia.
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 11/13
1999.
15. Rocha GA, Rocha EJ, Martins CV. The effects of hospitalization on the nutritional status of children. JPediatr (Rio J). Jan-Feb 2006;82(1):70-4. [Medline].
16. Marteletti O, Caldari D, Guimber D, Mention K, Michaud L, Gottrand F. [Malnutrition screening inhospitalized children: influence of the hospital unit on its management]. Arch Pediatr. Aug2005;12(8):1226-31. [Medline].
17. Oztrk Y, Buyukgebiz B, Arslan N, Ellidokuz H. Effects of hospital stay on nutritional anthropometric datain Turkish children. J Trop Pediatr. Jun 2003;49(3):189-90. [Medline].
18. World Health Organization. WHO Global Database on Child Growth and Malnutrition. Geneva: WHO.1996.
19. Kim Y, Hahn S, Garner P. Reduced osmolarity oral rehydration solution for treating dehydration causedby acute diarrhoea in children. Cochrane Database Syst Rev. 2001;(2):CD002847. [Medline].
20. UNICEF. New formulation of Oral Rehydration Salts (ORS) with reduced osmolarity. United NationsChildren's Fund. Available at http://www.supply.unicef.dk/catalogue/bulletin9.htm.
21. Plumpy'nut. Available at http://en.wikipedia.org/wiki/Plumpy'nut.
22. Joint Statement by the World Health Organization, the World Food Programme, the United NationsSystem Standing Committee on Nutrition and the United Nations Children's Fund. Community-BasedManagement of Severe Acute Malnutrition. May, 2007.
23. [Guideline] World Gastroenterology Organisation (WGO). WGO practice guideline: acute diarrhea. Mar2008;[Full Text].
24. Schwarz SM, Corredor J, Fisher-Medina J, Cohen J, Rabinowitz S. Diagnosis and treatment of feedingdisorders in children with developmental disabilities. Pediatrics. Sep 2001;108(3):671-6. [Medline].
25. Bhutta ZA, Ahmed T, Black RE, Cousens S, Dewey K, Giugliani E. What works? Interventions formaternal and child undernutrition and survival. Lancet. Feb 2 2008;371(9610):417-40. [Medline].
26. Ashworth A, Jackson A, Khanum S, Schofield C. Ten steps to recovery. Child Health Dialogue. 1996;10-2. [Medline].
27. Barennes H, Kahiatani F, Pussard E, et al. Intrarectal Quinimax (an association of Cinchona alkaloids) forthe treatment of Plasmodium falciparum malaria in children in Niger: efficacy and pharmacokinetics.Trans R Soc Trop Med Hyg. Jul-Aug 1995;89(4):418-21. [Medline].
28. Beaufrere B, Bresson JL, Briend A, et al. Protein and energy requirements in children with severemalnutrition. Application in a hospital environment for the treatment of malnutrition caused by deficientintake. Arch Pediatr. 1998;5(7):763- 71. [Medline].
29. Berkley J, Mwangi I, Griffiths K, et al. Assessment of severe malnutrition among hospitalized children inrural Kenya: comparison of weight for height and mid upper arm circumference. JAMA. Aug 32005;294(5):591-7. [Medline].
30. Briend A, Wojtyniak B, Rowland MG. Arm circumference and other factors in children at high risk of deathin rural Bangladesh. Lancet. Sep 26 1987;2(8561):725-8. [Medline].
31. Buchanan N. Drug kinetics in protein energy malnutrition. S Afr Med J. Mar 4 1978;53(9):327-30.[Medline].
32. Buchanan N. Effect of protein-energy malnutrition on drug metabolism in man. World Rev Nutr Diet.1984;43:129-39. [Medline].
33. Buchanan N, Eyberg C, Davis MD. Isoniazid pharmacokinetics in Kwashiorkor. S Afric Med J.1979;56(8):299-300. [Medline].
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 12/13
34. Buchanan N, Robinson R, Koornhof HJ, Eyberg C. Penicillin pharmacokinetics in kwashiorkor. Am J ClinNutr. Nov 1979;32(11):2233-6. [Medline].
35. El-Sayed HL, Nassar MF, Habib NM, et al. Structural and functional affection of the heart in proteinenergy malnutrition patients on admission and after nutritional recovery. Eur J Clin Nutr. Apr2006;60(4):502-10. [Medline].
36. Finch RG. Adverse reactions to antibiotics. In: Greenwood D, ed. Antimicrobial Chemotherapy. 4th ed.Oxford, England: Oxford University Press; 2000:200-11.
37. Golden M. The effects of malnutrition in the metabolism of children. Trans R Soc Trop Med Hyg.1988;82(1):3-6. [Medline].
38. Gomez F, Ramos Galvan R, Frenk S, et al. Mortality in second and third degree malnutrition. In: BullWorld Health Organ. 2000;78(10):1275-80. J Trop Ped and Afr Child Health. 1956;2:77. [Medline].
39. Grantham-McGregor S. A review of studies of the effect of severe malnutrition on mental development. JNutr. 1995;125:2233-8 S. [Medline].
40. Krishnaswamy K. Drug metabolism and pharmacokinetics in malnourished children. Clin Pharmacok inet.1989;17 Suppl 1:68-88. [Medline].
41. Listernick R, Christoffel K, Pace J, Chiaramonte J. Severe primary malnutrition in US children. Am J DisChild. Nov 1985;139(11):1157-60. [Medline].
42. Long J, World Health Organization. Management of severe malnutrition: a manual for physicians andsenior health workers. 1999.
43. Martorell R, Habicht J-P, Rivera JA. History and design of the INCAP Longitudinal Study (1969-77) and itsFollow-up (1988-89). J Nutr. 1995;125:1027-41 S. [Medline].
44. Mazouni SM, Guignard JP. [Malnutrition in children and the variability of drug effects]. Rev Med SuisseRomande. Dec 1996;116(12):965-9. [Medline].
45. Mehta S. Drug metabolism in the malnourished child. Nestle nutr workshop ser. 1988;19:329-38.
46. Mehta S, Nain CK, Sharma B, Mathur VS. Disposition of four drugs in malnourished children. Drug NutrInteract. 1982;1(3):205-11. [Medline].
47. Mehta S, Nain CK, Yadav D, et al. Disposition of acetaminophen in children with protein caloriemalnutrition. Int J Clin Pharmacol Ther Toxicol. Jun 1985;23(6):311-5. [Medline].
48. Merritt RJ, Suskind RM. Nutritional survey of hospitalized pediatric patients. Am J Clin Nutr. Jun1979;32(6):1320-5. [Medline].
49. Polasa K, Murthy KJ, Krishnaswamy K. Rifampicin kinetics in undernutrition. Br J Clin Pharmacol. Apr1984;17(4):481-4. [Medline].
50. Pollitt E. Developmental sequel from early nutritional deficiencies: conclusive and probability judgments. JNutr. Feb 2000;130(2S Suppl):350S-353S. [Medline].
51. Rumack BH, Holtzman J, Chase HP. Hepatic drug metabolism and protein malnutrition. J Pharmacol ExpTher. Sep 1973;186(3):441-6. [Medline].
52. Seth V, Beotra A, Bagga A, Seth S. Drug therapy in malnutrition. Indian Pediatr. Nov 1992;29(11):1341-6.[Medline].
53. Taketomo CK, Hodding JH, Kraus DM. Pediatric dosage handbook . 12th ed. Hudson, Ohio: Lexi CompInc; 2005.
54. Tolboom JJ. Management of severe malnutrition and diarrhea. J Pediatr Gastroenterol Nutr. Mar2000;30(3):346-8. [Medline].
-
9/24/13 Marasmus
emedicine.medscape.com/article/984496-overview 13/13
Medscape Reference 2011 WebMD, LLC
About MedscapePrivacy PolicyTerms of UseWebMDMedicineNeteMedicineHealthRxListWebMD CorporateHelp
All material on this website is protected by copyright, Copyright 1994-2013 by WebMD LLC.This website also contains material copyrighted by 3rd parties.DISCLAIMER: The content of this Website is not influenced by sponsors. The site is designed primarily for use by qualifiedphysicians and other medical professionals. The information contained herein should NOT be used as a substitute for theadvice of an appropriately qualified and licensed physician or other health care provider. The information provided here is foreducational and informational purposes only. In no way should it be considered as offering medical advice. Please checkwith a physician if you suspect you are ill.
Close
55. Waterlow JC. Classification and definition of protein-calorie malnutrition. Br Med J. Sep 21972;3(826):566-9. [Medline].
56. Yadav D. Disposition of acetaminophen in children with protein caloric malnutrition. Clin Pharmacol Ther.1985;23:311-5.